






Injuries to the elbow are common in childhood. The history and clinical examination are essential for ruling out fracture; proper views of the elbow are indispensable to determine the extent of the injury.
In children it is essential to recognize the four secondary ossification centers of the distal humerus: the capitellum, the medial and lateral epicondyles, and the trochlea. The usual order in which these centers appear and the age at which they become radiographically visible are important factors in the evaluation of injuries to the elbow in children. Displacement of any of these centers serves as a diagnostic indicator of the type of fracture or dislocation. For instance, the medial epicondyle always ossifies before the trochlea. If radiographic examination in a child between four and eight years of age reveals a bony structure in the region of the trochlea (before this center should appear), and shows no evidence of the ossification center of the medial epicondyle, it must be assumed that the ossification center of the medial epicondyle has been avulsed and displaced into the joint. (Figure 2)
The lateral view of the elbow also is important for evaluating the joint space, the olecranon process, and the anterior aspect of the radial head. It is limited, however, in the information it can provide, particularly with respect to the posterior half of the radial head and the coronoid process, because of the overlap of bony structures.
The lateral view in children can be used to assess possible joint luxation or fracture. The distal humerus in children has an angular appearance resembling a hockey stick, the angle of which normally measures approximately 140 degrees. Loss of this configuration occurs in a supracondylar fracture. If a line were drawn along the longitudinal axis of the proximal radius, it should pass through the center of the capitellum. If a line were drawn along the anterior cortex of the distal humerus extending downward through the articulation, it should intersect the middle third of the capitellum. (Figure 3)
Disruption of this relation serves as an important indication of the possible presence of fracture or dislocation. Finally, regardless of the age of the patient, displacement of the normal positions of the fat pads of the elbow also provides a useful diagnostic clue to the presence of fracture. Normally, the posterior fat pad, which lies deep in the olecranon fossa, is not visible on the lateral view. When it becomes visible and the anterior fat pad appears displaced (the positive fat pad sign), evaluation for a fracture mainly of the radial head should be undertaken.
This information should be useful in the evaluation of the elbow, particularly in children. If there is any question as to fracture, reasonable precautions should be taken to avoid any possible permanent damage to the elbow.
References
Greenspan, Adam. Orthopedic Radiology, 1988.
Deborah Pate, D.C., D.A.C.B.R.
San Diego, California
Editor's Note:
Dr. Pate's book, Case Studies in Chiropractic Radiology is now available through MPI's Preferred Reading and Viewing list. Please see pages xx, Part #T123 for further information on how to order your copy.
A) For the AP view of the elbow, the forearm is positioned supine on the cassette. B) The film in this projection demonstrates the medial and lateral epicondyles, the olecranon fossa, the capitellum, and the radial head. C) The secondary centers of ossification of the distal humerus usually appear in the following order: capitellum at one to two years, the medial epicondyle at four years, the trochlea at eight years and lateral epicondyle at ten years.
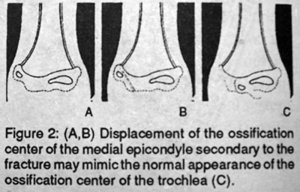
(A,B) Displacement of the ossification center of the medial epicondyle secondary to the fracture may mimic the normal appearance of the ossification center of the trochlea (C).
(A) For the lateral projection of the elbow, the forearm rests on its ulnar side on the cassette, with the joint flexed 90 degrees. (B) In children, the normal position of the capitellum relative to the distal humerus and proximal radius is determined by the position of the capitellum intersected by two lines: A line (a) coincident with the longitudinal axis of the proximal radius passes through the center of the capitellum, and a line (b) parallel to the anterior cortex of the distal humerus intersects the middle third of the capitellum. Disruption of this relation indicates the possible presence of abnormality.
Figure 4: For the radial head-capitellum view of the elbow, the patient is seated at the side of the table, with the forearm resting on its ulnar side, the elbow joint flexed 90 degrees, and the thumb pointing upward. The central ray is directed toward the radial head at a 45 degree angle to the forearm.
Click here for more information about Deborah Pate, DC, DACBR.