





Ouch! I just got zapped again in my left lumbopelvic (LP) region. Shocking pain and muscle failure caused me to drop to my knees. HVLA moves are painful and don't relieve the problem. I pull out my adjusting tool and go to town ... but only get temporary relief. Traction and stretching are irritating and uncomfortable to perform.
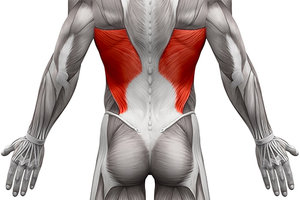
Who would have thought the lat could cause so much pain and immobility in my low back? Look closely at the distal insertion of the latissimus. It attaches to the spinous processes of L1 through L5 and into the superior aspect of the ilium.
When the left latissimus becomes hypertonic, it pulls the lumbar spinous processes up and to the left and pulls the ilium superior. This can create joint tension and locking of the SI and lumbars. It restricts pelvic elevation and lumbar lateral flexion.
Evaluation of the latissimus can be performed by testing muscle power output. Have the patient adduct their elbow into the rib cage. Next, stabilize the pelvis with one hand while you abduct the elbow with the other hand. Do not press the elbow up toward the armpit, as this will jam the humerus into the glenoid fossa and cause discomfort; as well as alter the findings of the muscle test. Use the same arc motion that the patient demonstrates during adduction and abduction to avoid joint jamming.
 Adjusting the lumbar spine and pelvis did little to relieve my issue, but addressing the belly of the muscle made a significant impact in eliminating this problem. Correction of the hypertonic fibers involved finding the most tender fibers in the belly of the muscle and holding them at a tolerable level. This moderate force allowed the muscle spindles to adapt to the stimuli without triggering a guarding response.
Adjusting the lumbar spine and pelvis did little to relieve my issue, but addressing the belly of the muscle made a significant impact in eliminating this problem. Correction of the hypertonic fibers involved finding the most tender fibers in the belly of the muscle and holding them at a tolerable level. This moderate force allowed the muscle spindles to adapt to the stimuli without triggering a guarding response.
- Patient position: prone, squeezing elbow into the ribs
- Doctor stance: standing beside patient
- Hand position: superior hand stabilizes the pelvis; inferior hand contacts the elbow
- Line of drive: pull elbow away from the body in an arcing manner
- Observe: do not jam the elbow up into the shoulder joint
While maintaining tolerable pressure into the muscle belly fibers, I was able to perform lumbopelvic movements in all directions, and unlock the lumbar and sacroiliac joints.
How did this problem begin? I was spearfishing and swimming against the current one day and then lifted a 50-pound bag in my right hand and carried it about 30 yards the next day. That evening, my low back muscles began to tighten. When I woke up, my back was painful and immobile.
I evaluated my limited range of motion and palpated the muscles and bones, looking for the answer in that region. The obliques, quadratus lumborum and spinal erectors were slightly tight and tender, and offered little relief when worked on. Even the latissimus insertions were somewhat tender, but did not make a significant difference.
I hope this insight will assist you in helping low back pain patients find pain relief and restore mobility. Include the latissimus analysis in your back pain protocols and discover more ways to treat patients effectively.
Dr. Todd Turnbull, has authored online courses and articles about concussions, sports performance, soft-tissue diagnosis, rehabilitation and disc herniations. He is a 1991 graduate of Life University, a board-certified chiropractic sports physician, and maintains a private practice in Portland, Ore. He can be contacted with questions or comments via his Web site: www.drtoddturnbull.com/DCJournal.