





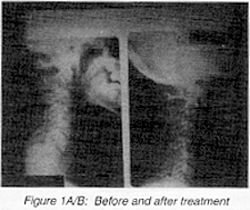
Figure 1A/B: Before and after treatment

Figure 2A: Before treatment
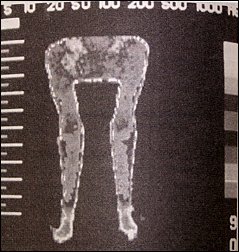
Figure 2B: After treatment
Chiropractic care is very efficacious for the management of many sports injuries.
However, it is in the subacute and later stages of rehabilitation where our strength lies, and where we make a big difference. It is in these stages of care where myofascial release technics are used to reduce myofascial adhesions and trigger points; where manipulative/adjustive technics are used to reduce joint dysfunction and restore normal biomechanics and kinematics to the athlete. Sport specific rehabilitation exercises are given as well as proprioceptive exercises so that the athlete can return to competition without compromise or fear of re-injury.
This article will focus on an injury to a high school football player during a game. This paper was presented about one and a half years ago at the annual meetings of the American College of Sports Medicine, and the FCER's ICSM Conference.
A 16-year-old football player who sustained a hyperflexion cervical injury, complained of neck pain, stiffness, and referred pain into the shoulder and upper arm area. Subsequent radiographs revealed no evidence of fracture or facet dislocation, however they did reveal a kyphotic cervical spine, anterior subluxation at C3/C4, and ligamentous instability in flexion/extension stress views with both abnormal translation and angular rotational displacement. Over a four week period the patient was treated, initially with rest, ice, physiotherapy, and a collar and in the subacute stages with myofascial and adjustive technics to the cervical spine.
The athlete responded quickly to care and returned to competition within three to four weeks of his injury. Posttreatment stress radiographs and pre/postthermographic scans, and clinical evaluation were used to objectively determine return to sports date. Figures 1 A/B and 2 A and B show the before and after radiographs and thermograms displaying the efficacy of his treatment in this case. The radiographs show a reduction of the kyphotic cervical spine, anterior subluxation, and the ligamentous instability. The thermography scans show a cessation of the somatosympathetic pathophysiology associated with myofascial and articular insult. The patient was followed up on at three months, six months, and one year. All x-rays showed continued stability and lordosis of the cervical spine. The patient continued to play interscholastic sports, without incident or re-injury.
David BenEliyahu, DC, CCSP, DNBCT
Selden, New York