






The impingement syndrome is a frequently overlooked but important cause of chronic shoulder pain and disability. Impingement occurs when there is encroachment on the subacromial space with loss of the normal sliding mechanism between the superior periarticular soft tissues of the glenohumeral joint and the coracoacromial arch.

Clinically, the impingement syndrome is seen in two main groups of patients. In young athletic patients involved in sporting activities in which frequent and repetitive overhead throwing motions are used (i.e., baseball, football, tennis), the onset of symptomatic impingement frequently occurs before 25 years of age. A second group consists of older patients in whom symptoms may appear spontaneously or in association with sporting activities (golf, tennis) or occupational stresses.
The impingement syndrome is characterized by sharp pain associated with abduction 70-120 degrees, external rotation 20-30 degrees, and internal rotation greater than 30 degrees. Classically, a full range of shoulder motion is present. The severity of the discomfort varies from mildly irritating to totally debilitating. On physical examination, crepitance may be palpated over the superior aspect of the shoulder at the point of impingement. Radiographic evaluation will demonstrate the presence of bony excrescences arising from the anteroinferior aspect of the acromion (subacromial spur) and sclerosis of the greater tuberosity of the humerus. Magnetic resonance imaging (MRI) will demonstrate changes in the supraspinatus tendon and many times there will be evidence of swelling and fluid. If the clinical symptoms are present and a subacromial spur is demonstrable on the plain films, the only additional imaging modality that may be necessary is another plain film of the subacromial region in the anteroposterior projection, with an x-ray tube tilt of 15 degrees in the cephalad direction which would separate the posterior portion of the acromion allowing a better view of the spur. If a subacromial spur cannot be demonstrated and clinical symptoms still indicate an impingement syndrome, a MRI of the shoulder may be necessary to demonstrate the more subtle types of shoulder impingement syndrome.
The treatment of the impingement syndrome depends on the chronicity of the disorder and associated abnormalities. In many patients, especially young athletes, the syndrome is first recognized at the stage of rotator cuff tendinitis and will generally respond well with conservative care. In the more chronic cases in which large subacromial spurs have caused a rotator cuff tear, anterior acromioplasty may be required.
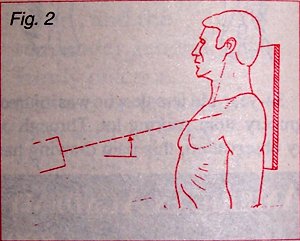
Diagram of the x-ray position for demonstrating the acromioclavicular joint and subacromial spur.
Deborah Pate, D.C., DACBR
San Diego, California
Click here for more information about Deborah Pate, DC, DACBR.