






When the sacroiliac (SI) joint is difficult to stabilize, it is also very difficult for the patient to heal. In chiropractic, this has been elegantly expressed in the SOT world. Unstable sacroiliacs are easy to adjust, with a satisfying, audible release; but in my experience, this doesn't change the outcome.
In my experience of motion palpation, the SI joint, even when unstable, can feel fixated and stuck. I suspect that the joint feels stuck because all of the muscles surrounding the joint are tight, trying desperately to keep the injured or dysfunctional joint as stable as possible.
What would lead us to suspect sacroiliac instability? 1. The patient continues to return with continued lower back or buttock pain. 2. The patient shows continued indicators for SI instability, such as a positive arm fossa test for SOT category 2, palpatory findings of pelvic sagittal rotation (AS or PI ilium), and/or bogginess and/or "ropiness" on palpating the SI joint itself. You may have different indicators for SI problems; feel free to use them. The bottom line is that the patient is not changing or responding. The first time he or she stresses the joint - when lifting, jogging, sitting, etc. - the joint subluxes again. I think we need to address the ligamentous and tendonous instability via actually restarting first-stage healing.
What is first-stage healing? When a ligament or tendon is injured, it goes through a process of inflammation and lays down new tissue. This inflammation is a necessary part of the first-stage healing. This is another good reason not to use NSAIDs after injury, as they block the first stage of the healing process.
In the unstable sacroiliac, first-stage healing has stopped. The muscular/tendonous component now has a tendinopathy. What is wrong with the tendons? I'll quote Warren Hammer: "What we really are seeing is an intratendinous degeneration due to aging, and microtrauma where there is collagen disorientation, disorganization and fiber separation."1
The ligament components have been studied less, but the problems are parallel, with degenerative changes leading to functional laxity. This can be hard to assess via joint mobility testing, as the muscles attempt to take over the stabilizing function and become tight.
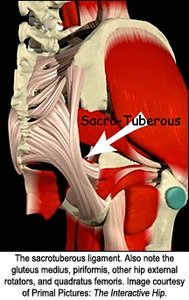
What ligaments and tendons tend to not be functional around the SI joint, and how should we assess and correct them? Let's break it down into four separate accessible ligaments. These include the sacrotuberous ligament, the sacrospinous ligaments, the iliolumbar ligaments, and the long posterior sacroiliac ligaments. All of these can be involved in SI instability.
Note that this palpation requires a pressure deep into the buttock region, often pushing through some fairly thick, soft tissue. This also involves touching an area that is rarely assessed, and that may be connected with old abuse memory patterns. Tell the patient what you are going to do, why you are assessing this area, and ask for their explicit permission. You may want to bring an assistant into the room; you may want to get an informed consent. Use good judgment.
I will use a broad definition of the sacrotuberous ligament, including the parts of the sacroiliac ligaments that interdigitate with it. Evaluate the sacrotuberous ligaments for tenderness with digital pressure along three areas, all at junctions of the ligament and bone: 1. Check the insertion of the sacrotuberous ligament along the ischial tuberosity and the ischial ramus. This is a large structure; you will need to palpate the whole of the medial side of the ischial tuberosity, pressing in a medial to lateral direction, looking for tender spots. 2. Check the sacral and coccygeal origin of the sacrotuberous. Here, your pressure needs to be primarily lateral to medial, pressing on the ligament's origin, from the lower sacrum down to the coccyx. 3. Check the extension superiorly of the origin of this ligament, from the PSIS and PIIS, from the posterior surface of the sacrum where it blends with the dorsal sacroiliac ligaments.
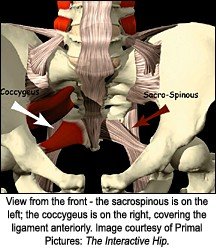
The sacrospinous ligament is continuous with the coccygeus muscle anteriorly. The only way I know to palpate this region accurately is to hook your index finger inferior to the sacrotuberous ligament, and then bring your hooked finger posterior. You will be up against the muscular aspect of the blended coccygeus and sacrospinous ligament. You can palpate the medial end of this ligament-muscle complex relatively easily at the anterior side of the inferior lateral angle of the sacrum, extending down toward the coccyx. Test for tenderness here, with lateral to medial pressure. Also move more laterally and assess for tenderness further along the belly of the muscle and ligament. You may be able to reach far enough laterally to feel the ischial spine, where these structures attach. Your test here would be to assess for tenderness with medial to lateral pressure.
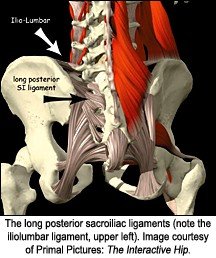
Next, check the iliolumbar ligament. This runs from the anterior superior surface of the ilium and iliac crest to the mammillary processes of the L4 and L5 vertebrae. It is a thickening of the thoracolumbar fascia. You may find tender points along the actual ligament, or along the whole of the fascial band. I have found more tenderness at the medial iliac crest. You can only palpate part of this ligament; some of it is positioned too deep anteriorly.
The most easily accessed ligaments of the SI are the long posterior sacroiliac ligaments. Palpate them in the joint space itself, going from the lateral sides of the sacrum to the medial ilium. Often only one or two spots will be tender in this region. Note the triangular arrangement of these ligaments, which resist downward motion of the sacrum on the ilium. The deeper fibers of the SI ligaments, the interosseous, are not directly palpable, due to the depth of the overall SI joint.
As you develop experience with this palpation, you will gradually get a sense of abnormal tissue texture, expressing as bogginess or excessive give, but for starters, tenderness is enough.
The tendons and muscles that need assessing include the gluteus maximus, especially its origins at the medial ilium; the gluteus medius origins; and the piriformis origin along the sacrum. Assess the whole superior and posterior aspect of the greater trochanter, the site of insertion of multiple buttock muscles. Assess the QL and the TFL. The quadratus femoris is often neglected. It acts as if it's a lateral extension of the sacrotuberous ligament. I will assume that most readers of this article are already familiar with these muscles and tendons, so I will not detail their anatomy or palpation. I will note that the same findings, that of tenderness on manual palpation and tissue texture changes, are good indicators of dysfunction.
How can you improve function in the ligaments and tendons, and at the musculotendonous junctions? Does your current treatment make a long-term difference, or just give temporary relief? Are you restarting first-stage healing? As I mentioned in my last article, I know of several methods to stimulate fibroblastic activity. The first would be cross-frictional massage. The second is Graston Technique. The third is prolotherapy injections of glucose and other solutions. All three of these initiate the inflammatory cascade and bring blood to the area. Other deep-tissue techniques, such as Nimmo or active release, may also have similar effects. [Editor's note: Dr. Heller's last article, "Chronic Sequelae of Ankle Sprains," appeared in the May 21, 2005 issue: www.chiroweb.com/archives/23/11/11.html.]
Now, I get to the tricky part: explaining the treatment. I basically have applied the principles and tools of the Graston Technique to these specific parts of the pelvis. I know most of you are not trained in Graston Technique, and don't have these metal tools. To apply these methods manually, use small-amplitude, manual cross-fiber massage and along-the-fiber, deep-tissue massage at the involved ligaments. For larger areas, your motions may be larger. This technique will be painful to the patient, but the pain should diminish as you continue. I tell my patients that if the pain becomes intolerable, (more than 6 on a 0-10 scale), to let me know, and I will back off. Manual cross-fiber methods recommend taking 5 to 10 minutes per local spot or area, and gradually increasing your pressure, as you create local anesthesia at various depths.2 When you are done, the areas should no longer be tender. My basic criteria for whether I am having success changes on follow-up in both symptoms and palpatory tenderness. Within a few treatments, the local areas of tenderness should diminish in both size and intensity.
Most of the research on restarting first-stage healing with manual therapies relates to the tendons, including Davidson's studies of rat tendons' response to Graston Technique.3 There is one good study I know of on the ligaments, by Klein, et al., using post-prolotherapy biopsy of the posterior sacroiliac
ligaments, showing fibroblastic hyperplasia and increases in ligament diameter.4 Use of cross-frictional massage or Graston Technique on ligaments is to some degree speculative, backed by a good understanding of the underlying physiology, but not well-proven by research studies using these specific modalities.
I'll share a brief case history. My interest in the sacrotuberous region started with a patient I was failing on. She had had two years of disabling groin pain, severe pain that kept her bedridden for weeks at a time, and that flared up from most bodywork. I had tried everything in my large toolbox, without any substantial change. I sat down with her and tried to figure out a new strategy. She pointed to her sacrotuberous ligament and said, "This is one of my most painful areas." I proceeded to examine the ligaments of her pelvis, as described above, and found significant tenderness and laxity in the sacrotuberous and sacrospinous ligaments. Having recently studied Graston Technique, I tried using these instruments, performing cross-frictional massage to these tender areas. She was significantly improved within a few sessions.
The other warning I will give about using these methods on any area is that the patient may be very sore. Cross friction, Graston Technique, and prolotherapy injections are all, in some sense, a carefully controlled bruising of the patient. In some sense, you are re-injuring the area in order to restart the healing. The patient may return literally bruised and complaining of extreme soreness. Start relatively gently, and slowly increase your treatment intensity. Warn the patient of possible responses, and frame these responses as part of the healing process.
This ligament work is not a complete and total solution for the sacroiliac. Use your usual low-force adjustment skills, and teach appropriate rehab and patient postural awareness. After 25 years, I find I still have much to learn about basic problems such as sacroiliac dysfunction. I hope this article helps you and your patients in the search for health.
References
- Goodbye, tendonitis, hello, tendinosis. Dynamic Chiropractic, July 24, 2000: www.chiroweb.com/archives/18/16/06.html.
- Hammer, W., in Functional Soft Tissue Examination and Treatment by Manual Methods, 2nd edition. Jones and Bartlett, 1999: chapter 14.
- Davidson CJ, Ganion L, Gehlsen G, et al. Morphologic and functional changes in rat Achilles tendon following collagenase injury and GASTM. Journal of the American College of Sports Medicine 1995;27(5).
- Klein, RG, Dorman TA, Johnson CE. Proliferant injections for low back pain: histological changes of injected ligaments and objective measurements of lumbar spine mobility before and after treatment. J Neurol Orthop Med Surg 1998;10:141-144.
Click here for more information about Marc Heller, DC.