






Despite sharing a common tendon, the soleus and gastrocnemius muscles function independently during stance phase, with the soleus playing a crucial role in limiting knee flexion by controlling movement of the tibia relative to the ground, while the gastrocnemius opposes this action by simultaneously flexing the knee and hip.1
What Makes the Soleus Unique
The soleus is especially important during propulsion, as it generates a force of eight times body weight to propel the body forward.2 This contrasts with the gastrocnemius's ability to generate vertical forces of only three times body weight.2
The soleus's incredible strength comes from its large cross-sectional area. In a cadaveric study comparing muscle size and morphology, Japanese researchers showed that the soleus has 1.5 times more volume than the gastrocnemius, three times the volume of the tibialis posterior, and six times the volume of the flexor hallucis longus.3 (Fig. 1)
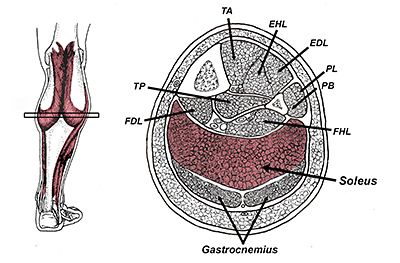 FIG 1 Cross-section demonstrating muscle volume and leg. Notice how the soleus is far and away the largest muscle below the knee.
Additional research shows that unlike the gastrocnemius, which is comprised mostly of fast-twitch fibers,4 the soleus possesses nearly 100 percent slow-twitch muscle fibers,5 which is why it is so important in distance running.
FIG 1 Cross-section demonstrating muscle volume and leg. Notice how the soleus is far and away the largest muscle below the knee.
Additional research shows that unlike the gastrocnemius, which is comprised mostly of fast-twitch fibers,4 the soleus possesses nearly 100 percent slow-twitch muscle fibers,5 which is why it is so important in distance running.
The muscle fibers of the soleus have also been shown to lengthen at a slower rate than gastrocnemius muscle fibers,6 allowing the soleus to more efficiently store and return energy. All of this information explains why a recent MRI evaluation of muscle volume in high-level marathon runners discovered that the fastest distance runners have the largest soleus muscles.7 In this study, gastrocnemius volume had no correlation with running speed.
Importance in Injury Prevention
Besides being essential for fast distance running, the soleus is also important in the treatment and prevention of Achilles injuries. In an interesting ultrasound evaluation of injured Achilles tendons, Counsel, et al.,8 confirmed that the vast majority of Achilles injuries happen at the midportion of the deep surface of the Achilles tendon, which is where fascicles from the soleus pull with the greatest force. Apparently, variation in interfascicular sliding plays a huge role in the development of Achilles tendon injuries.
In an innovative study comparing force output between the gastrocnemius and soleus in runners presenting with midportion Achilles injuries, O'Neill, et al.,1 demonstrated that injured runners have large deficits in strength and endurance, which the authors relate primarily to soleus weakness. In fact, the authors measured strength bilaterally and determined that compared to healthy controls, the soleus muscle in individuals with Achilles tendinopathy is significantly weaker on both the symptomatic and asymptomatic side.
The clinical implication of this research is that soleus weakness precedes the Achilles tendinopathy and rehab exercises should be performed bilaterally. Soleus weakness may also explain why an MRI study of 149 calf injuries in elite Australian Football players revealed that 85 percent of calf strains occurred in the soleus.9 Even worse, more than 91 percent of reinjuries occurred in the soleus and these injuries took longer to heal than gastrocnemius injuries.
Moving up the kinetic chain, some great research has shown that the soleus plays a key role in preventing anterior cruciate ligament injuries. Because this muscle prevents anterior translation of the tibia relative to the femur, the soleus is capable of exerting a powerful posterior force to prevent stretching of the ACL during sport.10
To prove this, researchers from Australia calculated posterior shear force generated by all potential knee-stabilizing muscles and determined that by limiting anterior translation of the tibia, the soleus provides greater protection to the ACL than the medial hamstrings and biceps femoris.11 While every rehab specialist knows to strengthen the hamstring muscles in order to prevent ACL injuries, few ACL prevention programs incorporate soleus exercises.
The same Australian researchers proved the soleus muscle also plays an important role in preventing valgus collapse of the knee.11 By pulling the tibia posteriorly during initial ground contact, the soleus keeps the knee aligned while the gluteus medius and hip rotators prevent excessive internal femoral rotation.
Preventing valgus collapse is one of the most important aspects of gait rehab, but all too often clinicians overly focus on just the hip musculature.
Preventing Cognitive Decline?
In what I think is the most fascinating research on the soleus muscle, McCleod, et al.,12 showed that soleus activity may play an important role in preventing age-related cognitive decline. According to the authors, age-related cognitive impairment is strongly correlated with reduced cerebral blood flow.
The authors point out that between the ages of 30 and 70, cerebral blood flow declines 30-50 percent; and that even mild exercise can enhance cerebral circulation, thereby limiting the rate of cognitive decline.
Unfortunately, nearly two-thirds of adults over age 75 do not engage in any physical activity whatsoever, and to make matters worse, it is not uncommon for individuals over age 70 to spend more than 12 hours per day sitting.13
In order to maintain cerebral blood perfusion, muscle activity is necessary to increase venous return to the heart, which in turn enhances cardiac output. According to Padberg,14 the soleus muscles are the body's primary muscle pumps responsible for forcing the return of blood from the lower extremity to the heart.
To evaluate the potential relationship between soleus activity and cognition, McCleod12 used a mechanical stimulus to force the soleus muscle to contract for one hour daily for four months in hypotensive senior citizens. At the end of that time, compared to an untreated control group, the seniors who performed soleus exercises demonstrated marked improvements in cognitive performance during executive function tests.
How to Keep the Soleus Strong
Given the connection between soleus strength and running performance, ACL stress, Achilles injuries, valgus collapse and even cognitive performance, it is important to keep the soleus muscle as strong as possible, especially as we age. Maintaining soleus strength and endurance is especially important for masters' runners, as research shows that older runners slow down because of reduced force output in the calf muscles, not reductions in hip or knee force output.15
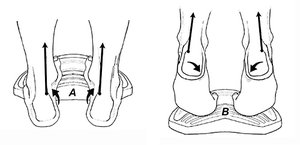 FIG 2 The medial fibers of the soleus play an important role in inverting the foot (A), while the lateral fibers are more active during rearfoot eversion (B).
My favorite way to strengthen the soleus is to perform four sets of 25 repetitions of bent-knee heel raises performed with the heel hanging off the edge of a step or foam platform. Because different fibers of the soleus are active when the foot is inverted or everted (Fig. 2), I have the patient actively invert and evert the rearfoot while performing heel raises.
FIG 2 The medial fibers of the soleus play an important role in inverting the foot (A), while the lateral fibers are more active during rearfoot eversion (B).
My favorite way to strengthen the soleus is to perform four sets of 25 repetitions of bent-knee heel raises performed with the heel hanging off the edge of a step or foam platform. Because different fibers of the soleus are active when the foot is inverted or everted (Fig. 2), I have the patient actively invert and evert the rearfoot while performing heel raises.
It is important to drop the heel down as much as possible, as exercising the soleus in a lengthened position produces significantly faster increases in strength, muscle volume and tendon resiliency.16-18 Also, when it comes to increasing muscle volume, the four sets of 25 light resistance exercise protocol has been proven to be just as effective as heavy resistance exercises,19 and the light resistance workouts are less likely to produce injury.
Whether you are treating biomechanical problems in elite athletes or inactive senior citizens with cognitive impairment, strengthening the soleus is often the key to effective treatment intervention.
References
- O'Neill S, Barry S, Watson P. Plantarflexor strength and endurance deficits associated with mid-portion Achilles tendinopathy: the role of soleus. Phys Ther Sport, 2019 May;37:69-76.
- Dorn T, Schache A, Pandy M. Muscular strategy shift in human running: dependence of running speed on hip and ankle muscle performance. J Exp Biol, 2012;215:1944-1956.
- Ito J, Moriyama H, Seiichiro S, et al. Human lower limb muscles: an evaluation of weight and fiber size. Okajimas Folia Anat Jpn, August 2003;80(2-3):47-56.
- Gollnick P, Sjödin B, Karlsson J, et al. Human soleus muscle: a comparison of fiber composition and enzyme activities with other leg muscles. Pflügers Arch Eur J Physiol, 1974;348:247-255.
- Fletchern JR, MacIntosh BR. Running economy from a muscle energetics perspective. Front Physiol, 2017;8:433.
- Lai A, Lichtwark G, Schache A, et al. Differences in in vivo muscle fascicle and tendon is tissue behavior between the ankle plantarflexors during running. Scand J Med Sci Sports, 2018 Jul;28(7):1828-1836.
- Kovács B, Kóbor I. Gyimes Z, et al. Lower leg muscle-tendon unit characteristics are related to a marathon running performance. Nature, 2020;10:17870.
- Counsel P, Comin J, Davenport M, Connell D. Pattern of fascicular involvement in midportion Achilles tendinopathy at ultrasound. Sports Health, 2015;7:424-428.
- Green B, Lin M, Schache A, et al. Calf muscle strain injuries in elite Australian football players: a descriptive epidemiological evaluation. Scand J Med Sci Sports, 2020 Jan;30(1):174-184.
- Elias J, Faust A, Chu Y, et al. The soleus muscle acts as an agonist for the anterior cruciate ligament: an in vitro experimental study. Am J Sports Med, 2003;31:241.
- Maniar N, Schache A, Pizzolato C, et al. Muscle contributions to tibiofemoral shear forces and valgus rotational joint movements during single leg drop landing. Scand J Med Sci Sports, 2020 Sep;30(9):1664-1674.
- McCleod K, Stromhaug A. Reversal of cognitive impairment in a hypotensive elderly population using a passive exercise intervention. Clin Interventions Aging, 2017;12:1859-1866.
- Diaz K, Howard V, Hutto B, et al. Patterns of sedentary behavior and mortality in U.S. middle-aged and older adults: a national cohort study. Ann Intern Med, 2017;167:465-475.
- Padberg F. The Physiology and Hemodynamics of the Normal Venous Circulation. In: Gloviczki P, Yao JST, editors. Handbook of Venous Disorders. 2nd Edition. London: Hodder Arnold, 2001: pp. 25-35.
- Paquette M, DeVita P, Williams D. Biomechanical implications of training volume and intensity in aging runners. Med Sci Sports Exerc, 2018 Mar;50(3):510-515.
- Goldmann J, Sanno M, Willwacher S, et al. The potential of toe flexor muscles to enhance performance. J Sports Sci, 2012;31:424-433.
- Noorkõiv, M, Nosaka, K, Blazevich, A. Neuromuscular adaptations associated with knee joint angle-specific force change. Med Sci Sports Exerc, 2014;46:1525-1537.
- Alegre L, Ferri-Morales A, Rodriguez-Casares R, et al. Effects of isometric training on the knee extensor moment-angle relationship and vastus lateralis muscle architecture. Eur J Appl Physiol, 2014;114:2437-2446.
- Burd N, West D, Staples A, et al. Low-load high-volume resistance exercise stimulates muscle protein synthesis more than high-load low-volume resistance exercise in young men. PLOS One, 2010;5(8):e12033.
Click here for more information about Thomas Michaud, DC.