






Most of us focus on the shoulder that is elevated, the obvious overactivity of the levator scapula, and the problems that creates. But few of us even look for the shoulder that is depressed and downwardly rotated.
In the past, we viewed the upper trap as hypertonic and an elevator of the shoulder. That pattern was seen as part of Janda's upper-crossed syndrome. As bodyworkers, we like to beat on the upper trap. I suspect that most of the time, we are either doing no good or at best, providing temporary relief.
What if we were wrong? What if the upper trapezius functions more as a stabilizer; what if its prime function is to horizontally adduct the acromioclavicular complex? What if its function is centrating the shoulder, adding to stability? The levator scapula can still be the scapegoat, the elevator muscle that shortens and lifts the shoulder. This is not a negation of Janda's concepts, it's just an update, a tweak.
I first learned this concept from Mark Comerford, PT.1 One of Comerford's main overall contributions, in my opinion, is in clarifying the difference between the phasic mobilizer muscles and the tonic stabilizer muscles. The upper trapezius, in his view, is a stabilizer. That means it functions at submaximal contraction levels (10-30 percent) over a long time. Stabilizers are inhibited by any pain, and mobilizers tend to get tight and upregulated by pain.
Anatomy of the Upper Trapezius
What evidence supports this newer concept of upper-trapezius function? "Anatomy and Actions of the Trapezius Muscle", by Johnson and Bogduk,2 looks at how the structure of the upper trapezius leads to its function. Warren Hammer wrote an excellent review article based on this, titled "The Upper Trapezius Does Not Elevate the Shoulder."3 For a deeper understanding of this anatomy, read Dr. Hammer's article and/or the Johnson / Bogduk article.
Johnson and Bogduk took a fresh look at the anatomy and probable function of the upper trapezius. They noted that the fibers of the upper trap reached the clavicle in an almost horizontal direction. The sweep of the cervical trapezius fibers passed downward and laterally, reaching the clavicle in an almost horizontal direction.
To quote Dr. Hammer's review,"The fascicles from the lower half of the ligamentum nuchae were much larger than the upper fibers. C6 and C7 fascicles were the largest and almost completely transverse." The orientation of the fascicles, except for those from the superior nuchal line, passed in more of a transverse than vertical direction to the clavicle. The upper fibers of the upper trap, coming from the upper neck, are much smaller and thus limited in their strength for elevation.
Based on this anatomy, what is the upper trap's action? It is to draw the clavicle backward or medially. The next question, which is what Comerford focused on, is what happens when the upper trap is weak? It allows the distal acromioclavicular complex to drop inferior, creating what Comerford calls a downward rotation of the scapula. Think of the triangle of the scapula, which should have a nearly horizontal top. Now imagine that the superior lateral corner is not supported and begins to drop inferior.
Let's take a look at the major scapular stabilization muscles. With our new view of the upper trap, we can see a three-part force couple. (Is that a force triplet?) The upper trap pulls the outer shoulder medially and the serratus draws the lateral inferior margin of the scapula forward, keeping the scapula against the chest wall. The middle and lower traps reinforce the medial pull of the upper trap and add an inferior pull.
Remember, these are all scapular stabilizers. They are not prime movers; they don't provide the power to throw or pull. Their important function is to stabilize, to hold the scapula in position to allow the bigger phasic muscles to function effectively from a solid base.
What other muscles contribute to a downwardly rotated scapula? The pectorals, when overactive, pull the shoulder inferior and anterior. An overactive latissimus dorsi may also contribute to this pattern.
Clinical Effects of Weak Stabilization Function of the Upper Trap
The next questions are: What are the clinical effects of the downward rotated scapula? What problems does a weak upper trap cause? There are two significant problems created by this scapular positioning. The first effect is in terms of function of the shoulder joint itself. When the glenoid fossa points inferior due to the scapular positioning, the shoulder will tend to get impinged. Imagine the humerus lifting from anatomical position into either flexion or abduction. If the glenoid points down, the humerus and the rotator cuff muscles above the humerus bang into the acromion arch much earlier. Voila: impingement.
Normalize the scapular position, fire the scapular stabilizer and the rotator cuff first as the arm lifts, and there is more room. Again, remember the function of the shoulder stabilizers. Both the upper trap and the whole rotator cuff are designed to set the shoulder, to centrate the shoulder, to properly position the shoulder to allow efficient function of the bigger muscles that pull and throw.
This concept does not take away from the concepts of anatomical impingement due to DJD or a type 2 or type 3 acromium. It does not negate the significance of weakness of the rotator-cuff muscles. It just helps complete the picture.
The second significant effect of upper-trap weakness and its posture affects the neck and the exiting nerve roots. The weight of the shoulder, unsupported by the stabilization from the upper trap, pulls downward. This creates a tension in the lower neck. Think of tension not in terms of emotion, but in terms of physics. Think of this tension as the upper trapezius and the whole lower neck on the involved side being passively stretched.
You can directly experience this. Actively depress and pull your shoulder inferior. Feel the tension in the lower neck and across the upper traps. Imagine what this does to the cervical nerve roots of a patient who is inflamed and already has less-than-optimal space for their nerve roots, due to DJD or a bulged cervical disc. What is the patient trying to do when they exhibit Bakody's sign, where the patient places their hand on their head? They are putting slack into the upper-trap region in order to take tension off of the nerve roots.
Why do the upper trapezius and the rotator-cuff muscles get inhibited? Our old friend, pain, is to blame again. Pain of any kind that affects the neck and/or shoulder girdle will shut down the stabilizer muscles. If the low back research can be extrapolated, it is likely that there will be some timing delay; delayed activation of the stabilizers. If the pain goes on long enough, you may see actual atrophy of the stabilizers. This is most palpable in the bulk of the infraspinatus, behind the scapula.
How Can We Correct Downward Rotation of the Scapula?
The primary solution is retraining the scapular stabilizer muscles, with emphasis on the upper trapezius. First, if your strategy has been to rehab the upper back by having the patient pull back and down, rethink this. You are potentially overactivating the lats. We don't want to train the scapula toward an inferior end range; we want it more neutral. Think of pulling straight back with various row-type exercises, with a high level of awareness of scapula positioning. Don't use the high-row style of back and down.
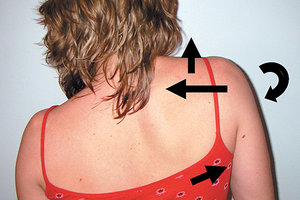
 Patient with left downward-rotated scapula. This is how your patient might present. Note that the left shoulder is low and the scapula is rotated downward.
Retraining the upper trap, getting the whole shoulder complex back to neutral, is tricky. The scapula is downwardly rotated, so we want to lift it. But the strategy is not elevation; the direction we want is a medial pull, an adduction toward the spine of the A-C area, using the strongest fibers of the upper trap. Remember, we are training a stabilizer, so we want longer holds, slow movement, and 10-30 percent of maximal effort.
Patient with left downward-rotated scapula. This is how your patient might present. Note that the left shoulder is low and the scapula is rotated downward.
Retraining the upper trap, getting the whole shoulder complex back to neutral, is tricky. The scapula is downwardly rotated, so we want to lift it. But the strategy is not elevation; the direction we want is a medial pull, an adduction toward the spine of the A-C area, using the strongest fibers of the upper trap. Remember, we are training a stabilizer, so we want longer holds, slow movement, and 10-30 percent of maximal effort.
Two specific exercise strategies work here. One is from Shirley Sahrmann, her upper-trap strengthening exercise.4 This is a bilateral exercise. See the pictures below.
For the first exercise, have the patient stand against a wall or door. For the start position, the arms are up, but bent at the elbow, and about 30 degrees out from vertical. The little finger is against the wall. From here, shrug the shoulders up and reach up with the hands. Hold this and squeeze the shoulder blades together; the hand and arm are pulled back away from the wall. Hold for 5-10 seconds, repeat 3-6 times, two times per day.
The second exercise is from Mark Comerford, et al. It is a little more mentally challenging, but gets to the essence of what we want. I tend to use these more cognitive exercises on patients who are open to subtlety, who are "in their body," and who are likely to succeed at this.
 Upper-trap subtle exercise: The goal is to upwardly rotate the previously downward-rotated scapula.
The idea is to suck the shoulder into its socket, gently pull the shoulder medially and hold. One of my cues is to ask the patient to "centrate" the shoulder. Patients seem to understand this verbiage. In doing so, you raise the height of the shoulder. The clinician needs to monitor and make sure the levator scap is not overfiring (the shoulder is not being elevated). Hold this position for 10 seconds, then relax for 2-3 seconds, and repeat up to 10 times, twice a day. The shoulder does end up in a weird-feeling position, up a bit higher than the opposite one. This is not the goal, just an overshoot to give the patient the experience.
Upper-trap subtle exercise: The goal is to upwardly rotate the previously downward-rotated scapula.
The idea is to suck the shoulder into its socket, gently pull the shoulder medially and hold. One of my cues is to ask the patient to "centrate" the shoulder. Patients seem to understand this verbiage. In doing so, you raise the height of the shoulder. The clinician needs to monitor and make sure the levator scap is not overfiring (the shoulder is not being elevated). Hold this position for 10 seconds, then relax for 2-3 seconds, and repeat up to 10 times, twice a day. The shoulder does end up in a weird-feeling position, up a bit higher than the opposite one. This is not the goal, just an overshoot to give the patient the experience.
I have placed a pdf of this exercise on my website at http://sosas.us/patient-resources/exercises. Feel free to print it out and use it in your office.
Taping also can be useful; the tape is designed to pull the acromioclavicular region medially. You can use McConnell taping, as that style of taping absolutely holds the shoulder in the new position. This is what Comerford teaches. I tend to prefer elastic therapeutic-type taping here, as a proprioceptive stimulus.
Start medially, right over the ligamentum nuchae at C6-7 and go laterally to the top of the shoulder. I usually use two 2-inch strips, the second below the first. Remember that elastic tape pulls back from where it finishes. Some of the more traditional elastic-style tapings for the shoulder are appropriate here as well, as they tend to help suck the shoulder into its socket, reinforcing the rotator cuff.
You cannot solve this problem without rehab and awareness, but secondary treatment components may be useful. Assess and mobilize stuck segments in the lower cervical spine, upper thoracic spine and rib cage. An anterior-fixated lower cervical will shut down the shoulder muscles. The upper thoracic often gets stuck, and this can affect movement of the scapula. The second, third and fourth ribs, and their intercostals, are often fascially adhered in the axillary region. The levator scap and the rhomboids are often too tight and have fascial densities that need releasing.
Take another look at your shoulder and neck pain patients. You may be surprised at what you see when you look with new eyes.
References
- Comerford M. "Trapezius: Clearing up the Confusion." Webinar; for more information see MovementPerformanceSolutions.com.
- Johnson G, Bogduk N, Nowitzke A, House D. Anatomy and actions of the trapezius muscle. Clin Biomech, 1994:44-50.
- Hammer W. "The Upper Trapezius Does Not Elevate the Shoulder." Dynamic Chiropractic, Feb. 26, 2004.
- Sahrmann S. Diagnosis and Treatment of Movement Impairment Syndromes. Mosby, 2001: p. 445.
Click here for more information about Marc Heller, DC.