






Routine radiographic examination of the wrist is not difficult, but does require some attention to positioning.
The PA View
The PA radiograph of the wrist is best obtained with the arm abducted 90 degrees from the trunk and the forearm flexed 90 degrees at the elbow. The wrist should lie flat on the cassette with the hand in a relaxed position, but with the fingers slightly cupped or flexed, or curled in a relaxed fist. A wedge also can be placed underneath the fingers to keep the wrist in contact with the cassette. The thumb should be extended parallel to the other fingers. (Figure 1)
 Figure 1: PA wrist
The most common problem I've seen is that the PA projection is performed with the hand extended flat on the cassette, which elevates the wrist slightly, causing the carpals to appear jammed together. If the clinician instructs the patient to place their hand in a gentle fist position, this will help place the carpal bones of the wrist closer to the cassette. (Figure 2)
Figure 1: PA wrist
The most common problem I've seen is that the PA projection is performed with the hand extended flat on the cassette, which elevates the wrist slightly, causing the carpals to appear jammed together. If the clinician instructs the patient to place their hand in a gentle fist position, this will help place the carpal bones of the wrist closer to the cassette. (Figure 2)
 Figure 2: PA wrist with hand in gentle fist
Technical factors that are important to keep in mind include the following: 10 x 12 inch (24 x 30 cm) crosswise for two or more images on one cassette; for a digital screen, use lead masking to get more than one image one the cassette; for a detail screen, use the tabletop technique; 50-60 kVp range, mAs 4-5; and minimum SID of 100 cm.
Figure 2: PA wrist with hand in gentle fist
Technical factors that are important to keep in mind include the following: 10 x 12 inch (24 x 30 cm) crosswise for two or more images on one cassette; for a digital screen, use lead masking to get more than one image one the cassette; for a detail screen, use the tabletop technique; 50-60 kVp range, mAs 4-5; and minimum SID of 100 cm.
 Figure 3: PA wrist
When evaluating the PA view of the wrist (Figure 3), the joint spaces of the wrist have a width of 2 mm or less. Only the radiocarpal joint is slightly wider. The carpometacarpal joints are slightly narrower than the midcarpal joints. The capitolunate joint is considered the baseline joint width to which other joint spaces can be compared. Make sure to look at all of them: the radiocarpal, the proximal intercarpal, the midcarpal, the distal intercarpal and the carpometacarpal joint spaces.
Figure 3: PA wrist
When evaluating the PA view of the wrist (Figure 3), the joint spaces of the wrist have a width of 2 mm or less. Only the radiocarpal joint is slightly wider. The carpometacarpal joints are slightly narrower than the midcarpal joints. The capitolunate joint is considered the baseline joint width to which other joint spaces can be compared. Make sure to look at all of them: the radiocarpal, the proximal intercarpal, the midcarpal, the distal intercarpal and the carpometacarpal joint spaces.
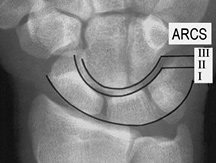 Figure 4: The carpal arcs
The carpal joint spaces should be symmetrical. The cortical margins of the bones should be parallel. One excellent way of looking at the positioning of the carpals is by using three carpal arcs. (Figure 4) The first arc is a smooth curve outlining the proximal convexity of the scaphoid, lunate and triquetrum. The second arc traces the distal concave surfaces of the same bones, and the third arc follows the main proximal curvatures of the capitate and the hamate.
Figure 4: The carpal arcs
The carpal joint spaces should be symmetrical. The cortical margins of the bones should be parallel. One excellent way of looking at the positioning of the carpals is by using three carpal arcs. (Figure 4) The first arc is a smooth curve outlining the proximal convexity of the scaphoid, lunate and triquetrum. The second arc traces the distal concave surfaces of the same bones, and the third arc follows the main proximal curvatures of the capitate and the hamate.
 Figure 5: The carpal bones: scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate and hamate
An arc is disrupted if it cannot be traced smoothly. A break in one of the arcs indicates a fracture or the disruption of a ligament leading to a subluxation or dislocation.
Figure 5: The carpal bones: scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate and hamate
An arc is disrupted if it cannot be traced smoothly. A break in one of the arcs indicates a fracture or the disruption of a ligament leading to a subluxation or dislocation.
Here's a common board question: What's the most commonly fractured bone in the body? Ah, I'll bet you thought it was the scaphoid. It's actually the clavicle. But the most common region fractured is the wrist, with the scaphoid being the most commonly fractured wrist bone. (Trick question, matter of semantics, but what do you expect from a board exam?)
 Figure 6: Lateral wrist positioning
Can you remember the names of all the carpal bones? You've got the scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate and hamate. (Figure 5)
Figure 6: Lateral wrist positioning
Can you remember the names of all the carpal bones? You've got the scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate and hamate. (Figure 5)
The Lateral View
 Figure 7: Lateral view of the wrist
The lateral radiograph of the wrist is obtained with the arm adducted with the ulnar side of the forearm on the cassette. The elbow is flexed to 90 degrees, adjusting the hand and wrist to make certain they are in a true lateral position. The same technical factors can be used for the lateral projection as for the PA projection. (Figure 6) If an X-ray table is not available, any sturdy table will do. This is a non-bucky technique.
Figure 7: Lateral view of the wrist
The lateral radiograph of the wrist is obtained with the arm adducted with the ulnar side of the forearm on the cassette. The elbow is flexed to 90 degrees, adjusting the hand and wrist to make certain they are in a true lateral position. The same technical factors can be used for the lateral projection as for the PA projection. (Figure 6) If an X-ray table is not available, any sturdy table will do. This is a non-bucky technique.
 Figure 8: Position of the pisiform for the true lateral wrist projection
When evaluating the lateral view of the wrist (Figure 7), it is important to first determine if a true lateral view has been performed. A true lateral view is defined by the relationship between the pisiform, capitate and scaphoid bones. On a standard lateral view, the palmar cortex of the pisiform bone should overlie the central third of the interval between the palmar cortices of the distal scaphoid pole and the capitate head. (Figure 8)
Figure 8: Position of the pisiform for the true lateral wrist projection
When evaluating the lateral view of the wrist (Figure 7), it is important to first determine if a true lateral view has been performed. A true lateral view is defined by the relationship between the pisiform, capitate and scaphoid bones. On a standard lateral view, the palmar cortex of the pisiform bone should overlie the central third of the interval between the palmar cortices of the distal scaphoid pole and the capitate head. (Figure 8)
Once it's been determined that a true lateral projection has been obtained, the spatial relationships between the carpal bones can be evaluated. The most important axes are those through the scaphoid, the lunate and the capitate. The true axis of the scaphoid is difficult to appreciate since the midpoint of the proximal pole is often not visualized clearly, but a parallel line can be used to determine if the scaphoid is spatially aligned. Drawing a line along the most ventral points of the proximal and distal poles of the scaphoid will achieve the same spatial relationship. (Figure 9)
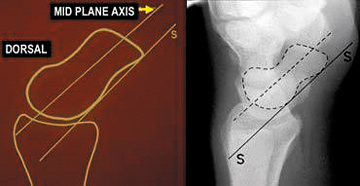 Figure 9: Axis of the scaphoid
The axis of the lunate runs through the midpoints of the convex proximal and concave distal joint surfaces, and can best be drawn by finding the perpendicular to a line joining the distal palmar and dorsal borders of the bone. (Figure 10) The capitate axis joins the midportion of the proximal convexity of the third metacarpal and that of the proximal surface of the capitate. (Figure 11)
Figure 9: Axis of the scaphoid
The axis of the lunate runs through the midpoints of the convex proximal and concave distal joint surfaces, and can best be drawn by finding the perpendicular to a line joining the distal palmar and dorsal borders of the bone. (Figure 10) The capitate axis joins the midportion of the proximal convexity of the third metacarpal and that of the proximal surface of the capitate. (Figure 11)
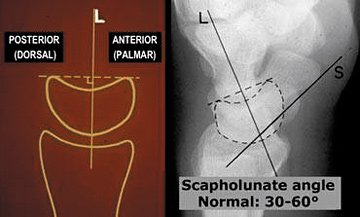 Figure 10: Axis of the lunate
Since we are discussing the lateral view of the wrist, we can't ignore the most commonly luxating/dislocating bone in the body, which is the lunate. Scapholunate instability can be assessed in the lateral view by measuring the scapholunate angle (30-60 degrees is normal – Figure 10) and the capitolunate angle (<30 degrees is normal – Figure 11). If the lunate is angulated dorsally, it is termed a DISI type of instability, which stands for dorsal intercalated segmental instability. Most agree that anything over 80 degrees for the scapholunate angle indicates instability. As far as VISI, volar intercalated segmental instability, or palmar flexion instability, when the lunate is tilted palmarly too much, most agree that VISI cases are most likely a normal variant, especially if the wrist is very lax.
Figure 10: Axis of the lunate
Since we are discussing the lateral view of the wrist, we can't ignore the most commonly luxating/dislocating bone in the body, which is the lunate. Scapholunate instability can be assessed in the lateral view by measuring the scapholunate angle (30-60 degrees is normal – Figure 10) and the capitolunate angle (<30 degrees is normal – Figure 11). If the lunate is angulated dorsally, it is termed a DISI type of instability, which stands for dorsal intercalated segmental instability. Most agree that anything over 80 degrees for the scapholunate angle indicates instability. As far as VISI, volar intercalated segmental instability, or palmar flexion instability, when the lunate is tilted palmarly too much, most agree that VISI cases are most likely a normal variant, especially if the wrist is very lax.
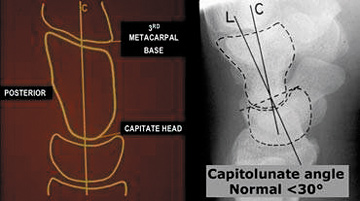 Figure 11: Axis of the capitate
The Oblique View
Figure 11: Axis of the capitate
The Oblique View
The other common view performed in a wrist series is the oblique view, which allows for visualization of the trapezio-trapezoidal joint. Again, this is a tabletop film. The patient is seated with the elbow flexed 90 degrees and the hand/wrist supinated. The fingers and hand should be slightly flexed to align the carpal bones. Rotate the wrist and hand internally 45 degrees toward the cassette; a 45 degree angle sponge can be used for support and stability. (Figure 12)
 Figure 12: Oblique wrist
Other Considerations
Figure 12: Oblique wrist
Other Considerations
 Figure 13: Oblique wrist demonstrating the trapezio-trapoidal joint
Functional views can also be performed if there is a question of ligamentous injury. Radial and ulnar deviation projections place stress on the intercarpal ligaments, which is used most often to evaluate the scaphoid bone. The clenched-fist PA wrist view can be also used to demonstrate a widening of the scapholunate distance.
Figure 13: Oblique wrist demonstrating the trapezio-trapoidal joint
Functional views can also be performed if there is a question of ligamentous injury. Radial and ulnar deviation projections place stress on the intercarpal ligaments, which is used most often to evaluate the scaphoid bone. The clenched-fist PA wrist view can be also used to demonstrate a widening of the scapholunate distance.
Wrist injuries are common and may lead to degenerative joint disease, which can prove debilitating. A simple wrist series can be quite helpful in evaluating most acute wrist injuries.
Click here for more information about Deborah Pate, DC, DACBR.