






Never having met a chiropractor who defended cervical kyphosis, I must ask myself the following question: against whom is this passionate defense of lordosis directed? Apparently, the few authors who suggest "that kyphotic cervical curvatures [sic] are 'probably a normal variant'" have "led many in the chiropractic profession to reject the notion of attempting to rehabilitate a patient's spine to some 'normal' anatomic configuration in favor of the clinical goal of absence of symptoms as the sole measure of clinical success." Yeah, whole legions of them.
This is very strange talk coming from a milieu which for many years has been so indifferent to patients' needs that they have demanded, in the most strident terms imaginable, that chiropractors eschew pain-reduction in a clinical setting where up to 95 percent of the patients come in with pain as their chief complaint. Doctors were to instead rack the patient's spines (at whatever expense, no matter how many years it took) into the quite impossible configuration of the Harrison spinal model, the doctor's primary measure of clinical success. As a compassionate chiropractor quite proud of being in the pain-reduction business, and with some considerable degree of success over the years, I have always pitied the patients (especially the asymptomatics) with reasonably normal lordotic necks who were being told they needed 60o lordoses, suffered from imagined "anterior weight bearing," needed a 30o atlas plane line, and so on. I have always wondered just how much "spinal reconstructive care" it would take to cram normal patients into the Harrison spinal model. No wonder all the boasting about "patient retention rates."
Dr. Harrison et al., invent these straw dogs all those chiropractors marching around in a pro-kyphotic trance, concerned only with symptom reduction because normative studies have compelled them to lay off their previous foils, those doctors who rejected (more typically, ignored) the hyperlordotic adventures of the Chiropractic Biophysics Technique. It seems that the only element common to both the old and the new Harrison spinal models is that the bad guys always come in 23o below the CBP estimate of the normal cervical lordotic angle.
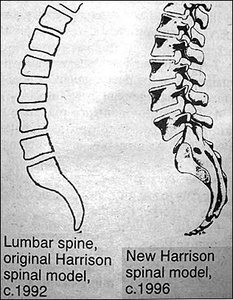
According to the most recent edition of the Chiropractic Biophysics tabloid,3 Dr. Harrison and others have submitted a paper to Spine in which they discover that 65 percent of the lumbar lordosis is concentrated from L4 to S1, and the upper lumbar spine is only minimally lordotic. Oh? My 1980 edition of Gray's Anatomy,4 which I have always regarded to be a higher authority than the Harrison spinal model, states: "The lumbar curve is convex forwards ... and the convexity of the lower three segments is greater than that of the upper two." After some 15 years of absurdly demanding the lumbar spine comprise a 60o arc from L1 to L5, the investigators are now willing to acknowledge that the spinal drawing which appears in practically every anatomy book and osteological chart is more anatomically correct than their own. Although it is good that Dr. Harrison et al., after having failed for so many years to foist their lumbar spinal model upon the rest of us, are now waking up from a self-imposed hyperlordotic nightmare, it is important that this level of imposture not go unnoticed. They should not be allowed to put their tag "Harrison Spinal Model" on all these other drawings, like chiropractic graffiti artists trying to stake out spinal territory (see figure).
Finally, it is reassuring to note that in the new Harrison model, empirical studies represent the gold standard for what is "normal." The lumbar spine mensuration paper submitted to Spine "analyzes the lumbar curvatures [sic] of 50 healthy [do you mean asymptomatic?!] individuals on lateral lumbar radiographs." That's a lot better than relying upon the abstruse and unsupported mathematical formulas we have previously seen: the Pettibonesque and discarded "chord length=radius" model, the unreferenced Delmas index, and the bizarre lever arm/bending moment compromise suggestion.5 Now that Dr. Harrison no longer feels compelled to come up with the number 60o, a number that was simply assumed from the start, he is finally free to characterize patients as they are.
Nevertheless, he still believes it is important to present a geometric model that predicts the sagittal cervical curve. Time will tell whether it holds up as well as the Ptolemean description of the universe. In the meantime, it is indeed more methodologically sound, and certainly much kinder to patients, to fit a curve to their necks than to fit their necks to a curve. That truly marks a turning point for the Harrison spinal model, the moment when real patients are no longer excluded from it; indeed, when the model no longer exists as such. Now that we have seen reform in the sagittal plane, there is reason to hope that in the future Dr. Harrison et al., will no longer compel patients to be perfectly straight in the frontal plane, as he told me they must, at the Washington Centennial. Nothing is more predictable than that someday the gang will be back to tell us that mensuration of healthy subjects in the frontal plane showed some degree of mean physiological curvature that is apparently well-tolerated. Only they will be surprised. In the meantime, the mechanobabble continues, something like: "The AP spine must be perfectly straight, as any biomechanist will tell you, because engineering and physics principles tell us that ..."
ABS Meeting in December
The American Back Society, whose conferences I have covered for several years, will host its Fall meeting in San Francisco, December 12-14. This meeting will present the most current results of outcome studies from both the United States and Canada on the diagnosis and treatment of back pain. For further information, you may contact the American Back Society at 2647 E. 14th St., Suite 401, Oakland CA 94601, Tel (510)536-9929, Fax (510)536-1812.
References
- Harrison DD, Troyanovich SJ, Harrison DE, Janik TJ, Murphy DJ. A normal sagittal spinal configuration: a desirable clinical outcome. Journal of Manipulative and Physiological Therapeutics 1996;19(6):398-405.
- Harrison DD. Chiropractic Biophysics Phase I. Sunnyvale CA: Harrison Chiropractic Seminars, Inc., 1981.
- Harrison D. Rene Cailliet, MD co-authors lumbar spine paper with CBP. American Journal of Clinical Chiropractic 1996;6(3):1.
- Williams PL, Warwick R. Gray's Anatomy. (36 ed.) Philadelphia, PA: W.B. Saunders Company, 1980.
- Cooperstein R. Technique system overview: Chiropractic Biophysics Technique (CBP). Chiropractic Technique 1995;7(4):141-146.
Robert Cooperstein, MA, DC
Faculty member, Palmer West
E-mail:
Click here for previous articles by Robert Cooperstein, MA, DC.