






These symptoms are more often anterior shoulder pain but may even be posterior. There may be shoulder pain during active external rotation or concentric medial rotation. Testing the subscapularis with the arm abducted 90 degrees puts the shoulder in the impingement, which is not conducive to proper testing.
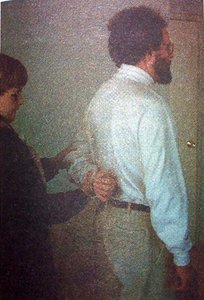
The life-off test is considered abnormal if there is an inability to move the hand off the back. The figure shows the examiner adding resistance against the forearm by which strength can be evaluated.
The subscapularis acts as a force coupled with the infraspinatus to help keep the humeral head centered on the glenoid throughout the entire range of shoulder motion. Weakness and pain in the subscapularis will allow upward displacement of the humeral head during motion and be responsible for possible shoulder impingement and instability. Its function as a dynamic internal rotator and depressor of the humeral head is essential for normal shoulder function. A very important function of the subscapularis is its eccentric activity protecting the shoulder during external rotation. Subscapularis eccentric activity shows more EMG activity than the concentrically contracting infraspinatus.1
A major problem in muscle testing is the simultaneous activation of muscle synergists. Testing the subscapularis in the neutral arm adducted position makes significant use of the synergistic pectoralis and latissimus muscles which, if normal, can easily substitute for a subscapularis tendinitis.
A lift-off test was originally devised by Gerber et al.2 to test for rupture of the subscapularis. Kelly et al.3 did EMG studies on the rotator cuff muscles and found that the lift-off test maximized subscapularis muscle activation and minimized the activation from the pectoralis and the latissimus muscles. Kelly also found that this test position, besides causing maximal activation of the muscle, allowed minimal activation of the synergists, good test-retest reliability, and decreased positional pain provocation.
The lift-off test is performed by having the standing patient put his/her arm behind the back with the dorsum of the hand on the midlumbar spine. Kelly et al.3 found that if the dorsum of the hand was at the buttock level, then the upper and lower subscapularis muscle tested one-third less. The patient pushes the hand off the back by maintaining or increasing internal rotation of the humerus and increasing extension at the shoulder. The elbow is kept at a constant flexion angle. The test is considered abnormal if there is an inability to move the hand off the back. The figure shows the examiner adding resistance against the forearm by which strength can be evaluated.
I have found this test to be present quite often when the usual neutral testing was negative. The only problem with performing this test is that the patient must possess full passive internal rotation without pain before attempting it. This test is an excellent way of determining equivocal subscapularis dysfunction.
References
- RM, Hawking RJR. Dynamic electromyographic analysis of the shoulder muscles during rotational and scapular strengthening exercises. In: Post M, Morrey BG, Hawkins RS. (eds.) Surgery of the Shoulder. St. Louis, CV Mosby, 1990.
- C, Krushell RJ. Isolated rupture of the tendon of the subscapularis muscle. Clinical features in 16 cases. J Bone Joint Surg 73B, 1991:389-394.
- BT, Kadrmas WR, Speer KP. The manual muscle examination for rotator cuff strength: an electromyographic investigation. Amer J of Sports Med 24(5), 1996:581-588.
Warren I. Hammer, MS, DC, DABCO
Norwalk, Connecticut
Click here for previous articles by Warren Hammer, MS, DC, DABCO.