






We are all aware of the fact that the annulus is innervated. It is the manner in which the disc is innervated that is the basis for the vertebrogenic pain caused by the injured disc. In the lumbar spine, somatic fiber originating for the recurrent meningeal nerve supply the posterior longitudinal ligament, the meninges, the blood vessels, the posterior extent of the outermost fibers of the annulus fibrosus, a portion of the periosteum of the vertebral bodies, and the underlying bone. In addition, a small branch from the ventral ramus of the somatic spinal nerve root directly innervates the posterolateral aspect of the vertebral body and adjacent tissues. Injury to any of these structures will incite well-circumscribed local somatic pain.1 Afferent pain fibers to the paraspinal sympathetic ganglia have been identified innervating the anterior and anterolateral disc and paravertebral structures including the anterior longitudinal ligament, the periosteum of the vertebral body, and the vertebral body itself.2 There is also a major sympathetic ganglion which joins the recurrent meningeal nerve.3 Therefore, the entire periphery of the disc is supplied with afferent sympathetic fibers.3
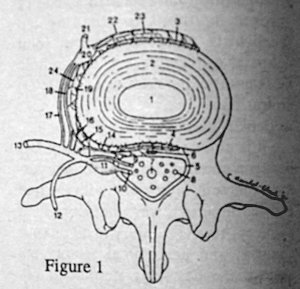
Schematic diagram of innervation of anterior spinal canal and structures of anterior aspect of spinal column (modified from 15-17): 1 = nucleus pulposus; 2 = annulus fibrosus; 3 = anterior longitudinal ligament/periosteum; 4 = posterior longitudinal ligament/periosteum; 5 = leptomeninges; 6 = epidural vasculature; 7 = filum terminale; 8 = intrathecal lumbosacral nerve root; 9 = ventral root; 10 = dorsal root; 11 = dorsal root ganglion; 12 = dorsal ramus of spinal nerve; 13 = ventral ramus of spinal nerve; 14 = recurrent meningeal nerve (sinuvertebral nerve of Luschka); 15 = autonomic (sympathetic) branch to recurrent meningeal nerve; 16 = direct somatic branch from ventral ramus of spinal nerve to lateral disk; 17 = white ramus communicans (not found caudal to L2); 18 = gray ramus communicans (multileval irregular lumbosacral distribution); 19 = lateral sympathetic efferent branches projecting from gray ramus communicans; 20 = paraspinal sympathetic ganglion (PSG); 21 = paraspinal sympathetic chain; 22 = anterior paraspinal afferent sympathetic ramus(i) projecting to PSG; 23 = anterior sympathetic efferent branches projecting from PSG; 24 = lateral paraspinal afferent sympathetic ramus(i) projecting to PSG. (Note: Afferent and efferent sympathetic paraspinous branches/rami may be partially combined in vivo.)
Because of the embryologic origin and anatomic pathways of the autonomic system, the conscious perception of somatogenic pain may result in appropriate localization of the symptomatology and the involvement of autonomic reflex functions. However, in general the pain is referred to the region corresponding roughly to the somatic distribution of the afferent fibers of the spinal nerve with which the afferent sympathetic fibers enter the spinal canal.3
The referred pain produces a nonspecific pain perceived in the low back as diffuse, deep, dull, and aching. This pain may also be referred to the lower extremities, however, it does not follow at dermatomal or scleratomal pattern.
This symptomatology has been referred to as the somatoautonomic syndrome.3 Further research is needed to aid in the recognition of this common but frequently misdiagosed problem.
References
- Edgar, M.A.; Ghadilly, J.A. "Innervation of the Lumbar Spine." Clin Orthop 1976; 115:35-41.
- Jackson, H.C.; Winkelman, R.K.; Binkel, W.H. "Nerve Endings in the Human Lumbar Spinal Column and Related Structures." J Bone and Joint Surg (Am) 1966; 14:475-489.
- Jinkins, J.R.; Whitemore, A.R.; Bradley, W.G. "The Anatomic Basis of Vertebrogenic Pain and the Autonomic Syndrome Associated with Lumbar Disc Extrusion." AJR June 1989; 152:1277-1289.
Deborah Pate, D.C., D.A.C.B.R.
San Diego, California
Editor's Note:
Dr. Pate's new book, Case Studies in Chiropractic Radiology is now available through MPI's Preferred Reading and Viewing list. Please see pages xx, Part #T123 for further information on how to order your copy.
Click here for more information about Deborah Pate, DC, DACBR.