






Patellar instability represents a wide range of problems, from microinstability to subluxation to gross dislocation. Although there are controversies regarding indications and timing for surgical treatment of recurrent patellar subluxation or chronic recurrent patellar dislocation, a patient who sustains an acute patellar subluxation or dislocation should consider orthopedic consultation.
Radiographs should be obtained, since up to 20 percent of patients demonstrate a radiographic loose body secondary to patellar instability. Osteochondral fractures of the patella may mimic patellar instability, demonstrating a loose body in the patellofemoral articulation on a radiograph. Patients may develop mechanical locking symptoms, necessitating arthroscopic removal of the loose body.
Once it has been determined that the problem is mainly the patellar subluxation, it is important to determine if it is a chronic condition or an acute single event.
Patients who have acute patellar subluxation or dislocation generally present with an episode of instability and have localized tenderness along the medial extensor retinaculum, or possibly at the adductor tubercle, which is the origin of the medial patellofemoral ligament. Also, the patient generally has localized tenderness along the peripheral edge of the lateral femoral condyle, where impaction from the patella occurs with flexion of the knee.
Acute patellar subluxation often appears no different from an acute patellar dislocation that has spontaneously reduced. Distinguishing one from the other is based on patient history. With a dislocation, the patient reports that the kneecap moved and had to be pushed back into place; with subluxation, the patient reports that the kneecap slipped out, and then went back into place spontaneously.
An acute patellar subluxation is generally not considered an indication for surgical treatment, and there are varied opinions with regard to the surgical indications for an acute patellar dislocation. Most sports medicine orthopedists treat acute patellar subluxations or dislocations in a closed fashion and emphasize a graded rehabilitation program after a period of immobilization. A palpable rent in the medial extensor mechanism, however, may be considered a surgical indication.
Patellar instability can occur in conjunction with ligamentous injuries about the knee. In particular, valgus mechanisms of injury resulting in a medial collateral ligament (MCL) sprain may also be associated with instability. Occasionally, acute patellar instability may occur in conjunction with an acute anterior cruciate ligament (ACL) injury. All of these ligamentous injuries should be assessed and determined if stable. If there is no associated ligamentous damage and no osteochondral fragment, the patient can be treated with conservative measures.
Another disorder that is often associated with patellar instability is chondromalacia patella. Technically, this means a softening or wearing away and cracking of the articular cartilage under the patella, resulting in pain and inflammation.
Unfortunately, the term "chondromalacia patella" is often used by physicians as a catch-all term to describe anterior knee pain that results from patellar malalignment. The most appropriate meaning is simply the degeneration of the cartilage on the posterior aspect of the kneecap. With abnormal repetitive motion due to muscle imbalance or biomechanical malalignment, the patella will rub irregularly on the femoral surfaces and the patellar articular cartilage will become irritated. The articular surface of the patella becomes inflamed and eventually will begin to degenerate. If caught early, this disorder can resolve with proper exercise and physical therapy.
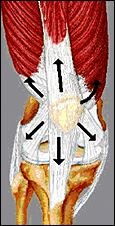
The primary function of the patella is to increase the efficiency of the quadriceps muscle by increasing its lever arm. This provides a mechanical advantage by lengthening the extension moment arm throughout the entire range of knee joint motion, but in doing so, it is subjected to considerable retropatellar compression force. Because of this biomechanical advantage, the patella is being acted upon by a number of factors during knee extension The fibers of the quadriceps muscles lie in different orientations and exert slightly different lines of pull on the patella. If one of the muscles is stronger or weaker than another, the imbalance can affect patellar tracking. The motion of the patella is also affected by the tightness or laxity of the medial and lateral patellar retinaculum, as well as by the iliotibial tract on the lateral aspect of the knee. All of these factors must be considered when examining a patient with patellar instability. It is mainly a tracking problem; if balanced, degenerative changes can be avoided.
The inflammation and degeneration of chondromalacia patella results from repetitive compression of the articular cartilage against the condyles of the femur following either an acute trauma or over an extended period of time. Normal patellar tracking allows motion of the patella through the trochlea of the femur without abnormal or excessive contact of the articular surfaces during knee extension. Malalignment of the patella can often result in abnormal forces and subsequent pathology.
An increase in the normal quadriceps angle (Q angle) of the knee may indicate a problem with internal rotation of femur. The Q angle is formed between a line drawn through the tibial tuberosity and the center of the patella, and another line drawn from the anterior superior iliac spine (ASIS) of the pelvis through the center of the patella.

The depth of the femoral groove and how the patella sits in this groove may also be causative factors in influencing the development of chondromalacia patella. The angle between the height of the medial and lateral femoral condyles, and the depth of the femoral groove, should also be assessed. If this angle is large, patellar motion can be excessive.
If the lateral structures are too tight and/or the medial structures are too loose, the patella will be pulled laterally. The patella will also track medially if the lateral structures are too loose and/or the medial structures are too tight. It is definitely a balancing act, and takes some time and patience to assess. The key here is to properly assess the cause of the imbalance, and rehabilitate the knee motion by strengthening and balancing the muscles involving the knee, particularly with extension.
Quadriceps strengthening may be the most important treatment once the pain has reduced. The muscular imbalance may be the direct cause of the patellar malalignment, and proper strengthening of the appropriate muscles can assist realignment of the patella and decrease or eliminate symptoms. As chiropractors, we are probably the most knowledgeable and in the best position to manage patellar instability, including chondromalacia patella.
Deborah Pate, DC, DACBR
San Diego, California
![]()
Click here for more information about Deborah Pate, DC, DACBR.