





Regrets, they say, are a waste of time. They are the past crippling us in the present. David Graston knows all about regrets and hasn't wasted a minute wallowing in them.
 He might have lost heart after suffering injuries that cost him the ability to compete as a semi-professional water-skier. And it would have been understandable had he lingered in depression after losing control over the instrument-assisted soft-tissue mobilization technique that bears his moniker, or succumbed to the seven-figure bankruptcy that ensued. Instead, at the juxtaposition of personal and profession ruin, David Graston sired sound-assisted soft-tissue mobilization (SASTM), the instruments and technique that many are calling the next generation in soft-tissue rehabilitation.
He might have lost heart after suffering injuries that cost him the ability to compete as a semi-professional water-skier. And it would have been understandable had he lingered in depression after losing control over the instrument-assisted soft-tissue mobilization technique that bears his moniker, or succumbed to the seven-figure bankruptcy that ensued. Instead, at the juxtaposition of personal and profession ruin, David Graston sired sound-assisted soft-tissue mobilization (SASTM), the instruments and technique that many are calling the next generation in soft-tissue rehabilitation.
Nearly five years after my introductory article on The Graston Technique, "The Promise of Tissue Remodeling" [March 26, 2001 DC], I decided to explore SASTM.
"I have utilized several types of instrument-assisted soft-tissue mobilization over the years, and these new SASTM instruments are indeed excellent," says Craig E. Morris, DC, DACRB, FAFICC. "For the patient, there seems to be less discomfort than with other methods I have used. For the treating doctor, there is less instrument slippage and more control. Instrument material and construct allow me to feel the tissues very well." Morris uses SASTM on his patients and has included it in the mobilization chapter of his new textbook, Low Back Syndromes: Integrated Clinical Management.
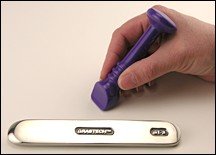
"Quite frankly, I'm surprised," says Morris. "I never expected to get the great outcomes I do from plastic."
 The "plastic" Morris refers to isn't your Toys R Us sort of plastic. The "plastic" in SASTM instruments is actually ceramic polymer. Historically, the material's relation to hard (rigidity) made widespread use cost-prohibitive to all but the aerospace industry. Research performed by Star Fire Systems in the late 1980s altered the molecular ratio of carbon to silicone, making it possible to customize viscosity and malleability, ultimately reducing the cost to machine it. Classified into one of three categories (structural ceramics, electronic ceramics, and high performance ceramic coatings), the material's affordability now is equaled only by its ability to marry customization to the end user.
The "plastic" Morris refers to isn't your Toys R Us sort of plastic. The "plastic" in SASTM instruments is actually ceramic polymer. Historically, the material's relation to hard (rigidity) made widespread use cost-prohibitive to all but the aerospace industry. Research performed by Star Fire Systems in the late 1980s altered the molecular ratio of carbon to silicone, making it possible to customize viscosity and malleability, ultimately reducing the cost to machine it. Classified into one of three categories (structural ceramics, electronic ceramics, and high performance ceramic coatings), the material's affordability now is equaled only by its ability to marry customization to the end user.
SASTM differs from its predecessors in three significant ways: instrument construct, instrument configuration, and instrument application. As a customized "structural ceramic," this material is known for its unmatched tensile strength, malleability and reverberation. Instrument configuration and application have changed, too. The rigidity of steel now yields to the flexibility of polymer. Convex and concave instruments designed to sweep around and treat amid anatomical prominences are replaced with blunt treatment edges specific to lesion size. Treatment edges decrease in size, as fibrotic lesions are isolated, treated and released. Pressure once disbursed along the entire instrument surface now is focused on and transmitted directly to the isolated lesion. "To increase treatment pressure to an isolated lesion with SASTM instruments, one would use an instrument with a smaller treatment surface area. The smaller focused treatment edge allows for deeper tissue penetration without the application of additional force by me," says Lawrence E. Jaggers, DC, LAc, FIAMA. (Adv), NMD.
 Graston is the creative force behind three of the contemporary instrument-assisted soft-tissue techniques currently on the market: augmented soft-tissue mobilization, (ASTYM), fashioned by Thomas L Sevier, MD, after a long collaboration with Graston; The Graston Technique; and SASTM. Graston and André Hall developed much of the methodology and technique used to identify and treat soft-tissue lesions. Essentially, each set of instruments is an amalgamation of the other, and all are derivatives of Graston's expertise and experience.
Graston is the creative force behind three of the contemporary instrument-assisted soft-tissue techniques currently on the market: augmented soft-tissue mobilization, (ASTYM), fashioned by Thomas L Sevier, MD, after a long collaboration with Graston; The Graston Technique; and SASTM. Graston and André Hall developed much of the methodology and technique used to identify and treat soft-tissue lesions. Essentially, each set of instruments is an amalgamation of the other, and all are derivatives of Graston's expertise and experience.
Grounded in the gua sha technique (pronounced "gwa shar") and long used in Chinese medicine, the SASTM instruments are a form of cross-fiber massage used to detect and break down areas exhibiting soft-tissue fibrosis or chronic inflammation. The microtrauma inflicted through the instrument initiates a healing cascade, and then ice and stretching are used help to quell pain, remodel tissue and restore function.
SASTM steps away from the historical blueprint for instrument-assisted techniques and into the realm of "fibrotic mapping." Treatment is focused on those areas or clusters of fibrotic tissue which directly relate to the symptomatic site without being the symptomatic site. SASTM does not initiate the inflammatory cascade (fibroblastic proliferation) at the symptomatic site or along the kinetic chain, as historically taught. Instead, microtrauma is applied to and within the corresponding "fibrotic map" in a systematic and sequential manner. "There are things that only became evident with the passage of time, and trial and error," says Graston.
A machinist by vocation and a trained tournament water-skier by avocation, Graston manufactured helicopter parts by night and trained for tournaments by day. In 1987, he suffered a life-altering injury when he dislocated his knee in a water-skiing accident. After reconstructive surgery and a long rehabilitation program, he was able to regain strength, but not range of motion. The therapist showed him how to perform cross-friction massage on the surgical scar (with his thumbs), which he found beneficial. Graston became "obsessed" with restoring motion to his knee and performed the cross-fiber massage continuously. Shortly thereafter, he was diagnosed with and surgercised for carpal tunnel syndrome. Thus began the construct and evolution of instrument and technique.
Steeped in need and fashioned from wood, Graston's first instrument design was a roller. "The wooden roller restored a modicum of motion to the surgical site, but did not allow me deep penetration into the tissues. Wood transitioned to aluminum, an affordable medium that provided penetrative abilities not found in the wood. Unfortunately, I still could not navigate around bony prominences," says Graston.
Through trial and error, instrument form followed function and the next generation of instruments was cast, first in aluminum and later in steel. Says Graston: "The steel instruments are great, they resonate beautifully, but the very material that allowed for reverberation increasingly became the origin of a grip problem. The cream used as a barrier between the instrument and the patient causes the steel to become slippery. Another byproduct of the instrument size and configuration is the unnecessary bruising of healthy tissue." SASTM treatment instruments are navigated by the shaft and held by "ridges" which prevent slippage while transferring vibrations from the treatment surface up the shaft and into the fingers. Instruments are designed around surface area; they are lesion specific and limit the intrinsic damage to surrounding healthy tissue.
Dale Buchberger, DC, DACBSP, ART, uses SASTM in his private practice (despite recently completing a research project at NYCC using the original Graston instruments). "SASTM instruments are easier on my hands, they don't slip and the treatment edges vibrate better in my hands. I find that the smaller the treatment edge, the greater the ability to isolate the lesion and the deeper the application of pressure.'Because treatment edges are lesion specific, there is almost no collateral damage to healthy tissue, or to me, for that matter. SASTM is just the next generation of instrument-assisted soft-tissue mobilization." says Buchberger.
"The incorporation of a microphone into some of the instruments can make even the best diagnostician better," says Doug Hayes, DC. "These instruments provide a direct conversation between the patient and their body. They provide a 'certainty' for what I suspect exists but what he patient could not experience otherwise. I am a musician as well as a doctor. You can play an ordinary guitar or you can play a Les Paul. They are the equivalent of isolating an individual 'note' in an entire song."
For 18 years, Graston has found himself in a continuous cycle of evaluation, adjustment and evolution of both instrument and technique. "We've learned a great deal in the past few years. For instance, historically we treated''symptoms' without necessarily getting to the origin of the problem. A perfect example is lateral epicondylitis. The symptoms for lateral epicondylitis may present in the elbow, and we would evaluate the symptomatic area and scan the kinetic chain, but the origin or cause of that condition is actually in the wrist and hand. We've found that symptoms and dysfunction are in place long before performance of the extensors becomes an issue. With SASTM, we no longer treat the symptoms or inflammation. We move away from inflammation and toward the adhesions or the source.
"Now I am not saying that there aren't adhesions in the inflamed tissue; there are. I am saying that they are'not the real problem. We've found that they are derivative lesions most likely developed secondary to the primary dysfunction which occurs elsewhere. Can you scan them, treat them and initiate a healing cascade? Yes, if you can find them through the inflammation and only to some degree. Over time, we've mapped 'patterns of fibrosis' that correspond to each condition. We've demystified the treatment and removed much of the unknown. We can now say that if symptoms present 'here' then go''there and there' and treat 'like this, and in this sequence.' When you initiate the healing cascade throughout the patterns of fibrosis in a sequential manner, there is an almost immediate and complete resolution at the symptomatic site."
The bottom line? Graston has developed a "best practice" model for instrument-assisted soft-tissue mobilization. "That" says Graston, "is the next generation."