






A few years ago, JAMA ran an editorial in which the writer advocated that health care practitioners, and in particular, general/family practitioners, should assume a responsible and leading position in educating their patients about the importance of automotive safety.
Information Shortfall
The author of this JAMA editorial correctly pointed out that Americans really don't receive sufficient or reliable safety information about their cars, other than warnings to buckle up. Even these warnings seem to fall often on deaf ears, judging by the fact that Americans are the least likely of all the world's citizens to use seat belts. Seat belts have historically been a major target of the government because they are such a critical safety feature and would very significantly reduce the number of fatalities and serious injuries if used by all. For those who elect to wear them, they will reduce serious injury or death in a severe crash by as much as 45 percent. This well exceeds airbag contributions to safety in frontal crashes, which is only about 12 percent by themselves (and only 5 percent when combined with belts).
After years of fruitless TV commercials and highway billboards exhorting us to use our seat belts, legislators finally discovered the real calculus motivating Americans: money. Primary and secondary seat belt laws quickly took the usage rate from less than 20 percent to more than 70 percent (only 10 percent to 19 percent of the population reported use in the 1960s) and generated some fine-based revenue in the process. And, good readers, it's not just our own safety about which we Americans are negligent. Parents were urged to use approved and age-appropriate child restraint systems (CRS) for children traveling in cars, but did they? Not more than a minority. Once again, legislation came to the rescue. The majority of states now have laws requiring CRS for children. A fine seems a more potent motivator than the mere thought of a maimed or deceased child. But in fairness to parents everywhere, most had never been told in earnest why the CRS was so important. Who has the responsibility for this?
Other Key Safety Features
I mentioned that frontal airbags surprisingly do not add much of a safety margin above and beyond seat belts in frontal crashes - and these are the airbags that all new cars have as standard equipment. Side-impact airbags, on the other hand, can provide much more safety margin in side impacts, but ironically, these are still optional equipment. Does the average car buyer understand the importance of side airbags or curtains? Given the choice, will they opt instead for the upgraded sound system and cool DVD player?
Electronic stability program (ESP), aka electronic stability control (ESC), is an electronic traction control that works with the antilock brake system to prevent loss of control. These are particularly effective in wet and icy conditions, and can decrease the number of crashes by as much as 45 percent. However, once again, this system (for the present) is also an option in most cars. However, like side airbags, ESP are so important that the Insurance Institure for Highway Safety will only award cars their coveted "Best Pick" award if the cars are equipped with ESP and side airbags.
One of the most important and least understood of the active safety systems is the child restraint system (CRS). This topic is complicated by the fact that these are a relatively recent development and the fact that there are four basic types, including booster seats (and many more models of each). These devices are not the simplest things to use, as evidenced by use studies that have indicated that as many as 89 percent of parents make one or more critical mistakes when placing their children in them. These critical errors could result in an otherwise avoidable serious injury or death of the child. In other cases, parents don't use CRS at all, in spite of the fact that motor vehicle crashes are the leading cause of preventable death and serious injury in children. Health care practitioners have a unique opportunity, and perhaps even a moral responsibility, to provide advice and encouragement to parents in the correct use of these systems.
Antilock brakes (ABS) were expected by most of us in the safety industry to greatly reduce collisions. Data showed, however, that their effect was not what we expected. The reason? People did not know how to use them and continued to apply the brakes tentatively as they were used to in cars with standard brakes where overzealous braking might cause wheel lockup and loss of steering control. With ABS, you apply very firm pressure (mash-and-pray) to maximize stopping power, without concern for wheel lock up. Are American motorists told how to optimally use these systems?
Head-Restraint and Seating Systems
Saving lives is certainly a high priority, but the rubric of automotive safety involves more than saving lives. It is also about preventing injuries that can rob us of the future quality of life. About 1 million people are injured so significantly in rear-impact crashes each year in the U.S. they will develop chronic neck pain and about 300,000 will become disabled. Much of this is preventable. Observational studies have repeatedly demonstrated, for example, that about 80 percent of vehicle occupants do not optimally adjust head restraints. And females, who are burdened with twice the risk for whiplash as males, are actually less likely to properly adjust these devices. Only about 20 percent of Americans take the time to place the head restraint into the optimal position. But how do they know to do this? Is it something you find in the car's owner manual? Are there highway billboards describing good head-restraint geometry? TV commercials? In all cases, the answer, of course, is no.
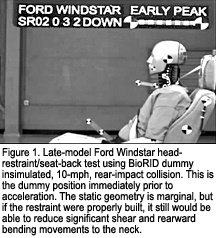 Head-restraint geometry is important, and to optimize it, the first step is to adjust the head restraint. However, many car seats have head restraints that are so poorly made that optimal geometry is difficult or impossible to achieve. Moreover, some cars have such poorly built restraints that they are virtually worthless, regardless. The Ford Windstar, for example, had restraints that were simply filled with foam and offered no real support to the head. This kind of callous disregard by manufacturers was what prompted the Insurance Institute for Highway Safety (IIHS) in 1995 to begin its head-restraint rating program. In the inaugural year, only 3 percent of the cars tested were given "good" ratings. Today this number is in the 50 percent range - still an indictment of the automakers' dissembling on safety issues. Essentially, if there is a federal requirement, they will comply with it. If a safety feature costs money and is not required, few American cars will have them. In 1969, a federal requirement mandated head restraints in passenger vehicles. So, in they went. But because there was no performance requirement built into the standard, all you had to do was place any bag of seat material filled with foam on the seat top and you were compliant with the rule. It didn't have to actually arrest a head in motion, as shown in Figure 1 and Figure 2.
Head-restraint geometry is important, and to optimize it, the first step is to adjust the head restraint. However, many car seats have head restraints that are so poorly made that optimal geometry is difficult or impossible to achieve. Moreover, some cars have such poorly built restraints that they are virtually worthless, regardless. The Ford Windstar, for example, had restraints that were simply filled with foam and offered no real support to the head. This kind of callous disregard by manufacturers was what prompted the Insurance Institute for Highway Safety (IIHS) in 1995 to begin its head-restraint rating program. In the inaugural year, only 3 percent of the cars tested were given "good" ratings. Today this number is in the 50 percent range - still an indictment of the automakers' dissembling on safety issues. Essentially, if there is a federal requirement, they will comply with it. If a safety feature costs money and is not required, few American cars will have them. In 1969, a federal requirement mandated head restraints in passenger vehicles. So, in they went. But because there was no performance requirement built into the standard, all you had to do was place any bag of seat material filled with foam on the seat top and you were compliant with the rule. It didn't have to actually arrest a head in motion, as shown in Figure 1 and Figure 2.
 This led to the IIHS developing a new standard a few years ago, which now is a two-part test. First, the seat and head restraint are tested for static head-restraint geometry. If it gets a "marginal" or "poor" rating, it's done. If it manages to get either an "acceptable" or "good" rating, it then goes on to the dynamic sled test, in which the seat is placed on a sled and a BioRID dummy is belted in and challenged to a simulated, 10-mph, rear-impact crash, as shown in Figure 1 and Figure 2. Ratings then depend on the dynamic performance recorded from internal instruments in the dummy. As with side airbags and ESP, the IIHS will now only award its "Best Pick" award to cars that have a "good" dynamic rating, as of this year. This should dispel any misconceptions that anyone might have concerning the insurance industry's ignorance of whiplash as a major public health problem or a "real" injury. In fact, the vanguard of whiplash research today is headed by the International Insurance Whiplash Protection Group (IIWPG), which is a consortium of the world's more influential insurance groups, including the IIHS.1 This should paint an interesting schizophrenic picture of the insurance industry. On the front line in corporate America, claims adjustors, doctors and lawyers pledging fealty to the insurance industry do their level best to dissuade Americans from believing in whiplash injury: the industry's long-time bête noir. Even television commercials feature subtle and not-so-subtle themes depicting rear-impact crashes as either trivial events or outright fraud. But behind the scenes, they know - perhaps better than anyone - the real size of the problem, and they want to fix it.
This led to the IIHS developing a new standard a few years ago, which now is a two-part test. First, the seat and head restraint are tested for static head-restraint geometry. If it gets a "marginal" or "poor" rating, it's done. If it manages to get either an "acceptable" or "good" rating, it then goes on to the dynamic sled test, in which the seat is placed on a sled and a BioRID dummy is belted in and challenged to a simulated, 10-mph, rear-impact crash, as shown in Figure 1 and Figure 2. Ratings then depend on the dynamic performance recorded from internal instruments in the dummy. As with side airbags and ESP, the IIHS will now only award its "Best Pick" award to cars that have a "good" dynamic rating, as of this year. This should dispel any misconceptions that anyone might have concerning the insurance industry's ignorance of whiplash as a major public health problem or a "real" injury. In fact, the vanguard of whiplash research today is headed by the International Insurance Whiplash Protection Group (IIWPG), which is a consortium of the world's more influential insurance groups, including the IIHS.1 This should paint an interesting schizophrenic picture of the insurance industry. On the front line in corporate America, claims adjustors, doctors and lawyers pledging fealty to the insurance industry do their level best to dissuade Americans from believing in whiplash injury: the industry's long-time bête noir. Even television commercials feature subtle and not-so-subtle themes depicting rear-impact crashes as either trivial events or outright fraud. But behind the scenes, they know - perhaps better than anyone - the real size of the problem, and they want to fix it.
Choosing a Safe Family Vehicle
Does the average motorist know how to translate the star-rating of the New Car Assessment Program (NCAP)? Do they understand that a five-star-rated subcompact is not as crashworthy as a five-star-rated midsized car? No, even though a description of the rating is available on the Internet and the rating is indicated on the window sticker. What about the IIHS' crash-test rating system? Even though they have recently tried to simplify it into a "Best Pick" rating, it still can be confusing, particularly because the NCAP and IIHS ratings sometimes conflict.
Many Americans believe that when it comes to crashworthiness, bigger is better. But this is only true in certain kinds of crashes, and we don't have the option of choosing our collision types. SUVs, which, more often than not, should stand for "seriously unnecessary vehicles," are more likely to roll over and more likely to leave the roadway in a crash. Their occupants are twice as likely to die in a rollover crash as compared to the occupants of passenger cars, which have a lower center of gravity, better road-handling ability and a shorter stopping distance.
I always counsel patients to consider their real needs first. If they need an SUV, start there. If they really don't need one, a minivan or passenger vehicle might be the better choice. Once the class of vehicle is determined, only then should they look into the various crashworthiness ratings. (Note: Truck, van, and SUV rollover ratings are another important consideration.) If patients have special risks, such as chronic neck disorders, prior surgical fusions, etc., then I would direct them to a vehicle equipped with whiplash-protection seats, such as the Saab or Volvo line. They are statistically more likely to be re-injured in a low-velocity crash without them.
Americans have few sources of quality and reliable information about automotive safety, but this education saves lives and the quality of life for millions every year. The logical first line of information is the family doctor. In fact, our position at the Spine Research Institute of San Diego is that this should really be an obligation of all physicians. For free information about public automotive safety, visit our Web site at www.srisd.com. The IIHS Web site is www.iihs.org, and the NHTSA Web site is www.nhtsa.gov. As always, I can be reached at
![]() .
.
Reference
- Croft AC, Freeman MD. Auto insurers and their new role in whiplash prevention - new rules, new risks, new tests. Forum;35(3):9-13.
Click here for previous articles by Arthur Croft, DC, MS, MPH, FACO.