






Plantar fasciitis is a degenerative condition in which repetitive microtrauma causes a structural breakdown of the connective tissue in the plantar fascia and/or neighboring muscles. In the United States alone, more than 1 million people receive treatment for plantar fasciitis annually.1
Challenging to Resolve
Until recently, it was assumed that the typical plantar fascial injury lasted about three months, and that only a small percent of the population, usually diabetics, developed chronic heel pain.
Using ultrasonography to evaluate 174 patients over 15-year period, the authors determined that 80 percent of plantar fascial patients had symptoms 12 months after the original injury, 50 percent had symptoms at five years, and a startling 44 percent had symptoms 15 years after the onset of their plantar fascial injury.
What's Causing Poor Outcomes?
 In my opinion, the terrible long-term outcomes reported in this study can be traced directly to the fact that the majority of people suffering with plantar fasciitis do not address the underlying biomechanical factors responsible for the development of the injury. While plantar fasciitis has been proven to correlate with weakness in the peroneal muscles of the leg and/or the intrinsic muscles of the arch, calf inflexibility is a common and significant cause of chronic plantar fasciitis.3
In my opinion, the terrible long-term outcomes reported in this study can be traced directly to the fact that the majority of people suffering with plantar fasciitis do not address the underlying biomechanical factors responsible for the development of the injury. While plantar fasciitis has been proven to correlate with weakness in the peroneal muscles of the leg and/or the intrinsic muscles of the arch, calf inflexibility is a common and significant cause of chronic plantar fasciitis.3
The reason calf inflexibility relates to the development of plantar fasciitis is that when the calf is tight, the heel is forced to leave the ground prematurely, transferring between three and five times body weight directly into the plantar fascia up to 10,000 times per day. Chronic calf tightness is problematic, as research over the past 20 years has repeatedly shown that stretching protocols, whether for the calf or any other muscle, tend to produce short-term length gains only, possibly explaining the high recurrence rates associated with plantar fasciitis.
Of all the muscles potentially responsible for limiting calf flexibility, tightness in the gastrocnemius has been proven to be the muscle most likely to cause plantar fasciitis. More than 20 years ago, DiGiovanni, et al.,4 confirmed that isolated contracture in the gastrocnemius muscle alone correlated strongly not just with plantar fasciitis, but also with a wide range of other foot injuries. In 2021, Pearce, et al.,5 demonstrated a strong correlation between the degree of gastrocnemius tightness and the severity of heel pain in plantar fascial patients.
What I find most interesting about gastrocnemius contracture is that it is not the entire gastrocnemius muscle that is responsible for producing plantar fascial pain; it is specifically the medial head of the gastrocnemius. This statement is supported by the fact that surgical release of the medial gastrocnemius produces an immediate 13 degree increase in ankle dorsiflexion6 and dramatically reduces chronic plantar fascial pain, producing better outcomes than when the plantar fascia is actually cut (plantar fasciotomy).7
Stretching: The Right Way
Rather than surgically sectioning the medial gastrocnemius muscle (or worse, cutting the plantar fascia), a less invasive approach for managing chronic plantar fasciitis is to lengthen the medial gastrocnemius with specific stretches. Until recently, experts suggested it is physically impossible to lengthen a muscle by stretching, as countless studies have shown that stretches produce only temporary improvements in flexibility and they in no way actually lengthen the muscle.
Fortunately, researchers from Greece and Austria8 noticed that prior to 2021, virtually all studies on the effects of stretching incorporated short-term stretching protocols in which stretches were performed for relatively short periods of time. These authors theorized that a high-volume stretching routine performed for an extended length of time would not only increase ankle range of motion, but also increase strength and performance.
The authors took 21 female athletes and had them perform two sets of six straight and bent-knee calf stretches, five times per week for 12 weeks. At the start of the study, each stretch was held for 45 seconds; the length of time each stretch was held was increased by 15 seconds every three weeks. Total stretch duration was nine minutes the first three weeks and 18 minutes for the final three weeks.
At the start and the end of the study, the authors used high-resolution photographs to measure ankle dorsiflexion, and ultrasonography was used to create panoramic sonograms to evaluate muscle fiber length and muscle cross-sectional area. Vertical jump height was also measured pre-and post-intervention by having the athletes perform a one-leg countermovement jump.
When the study was completed, the range of ankle dorsiflexion increased by 22 percent, muscle fiber length of the medial gastrocnemius increased 11 percent, cross-sectional area increased 23 percent, and one-legged jump height increased 27 percent.
The muscle head-specific changes in which the medial gastrocnemius lengthened more than the lateral gastrocnemius is particularly important for the management of plantar fasciitis, as lengthening the medial gastroc has a long history of successfully resolving plantar fascial pain.7 Importantly, the authors note that the improved range of ankle motion and cross-sectional muscle area were maintained even following detraining.
Clinical Implications
The clinical implication of this important paper is that short-term stretching protocols typically prescribed to treat plantar fasciitis need to be replaced with the high-volume stretching routines used in this study. In addition to increasing muscle cross-sectional area and improving jump height, the long-term stretching routine actually added more muscle fibers (sarcomeres) to the existing muscles, for the first time ever showing that it is possible to physically lengthen a muscle with stretches.
This research has implications not just for the management of chronic plantar fasciitis, but also for decreasing injury risk and/or improving performance in a wide range of activities.
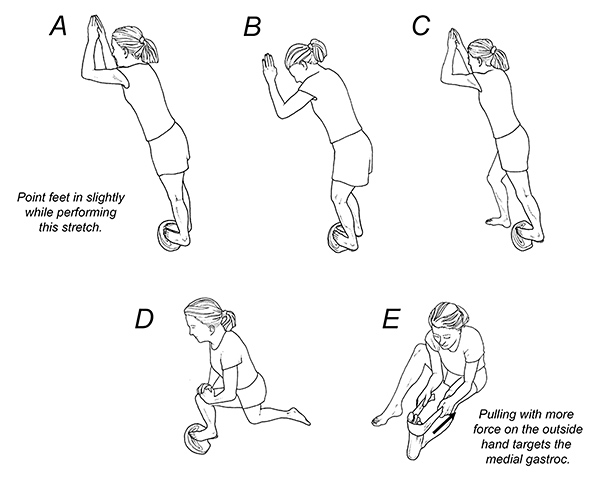
If you have patients dealing with chronic plantar fascial pain, or if you just want to help them make their tendons and muscles stronger, I highly recommend the stretches and exercises illustrated in Figure 1. According to the latest research, the prolonged stretches used in this protocol not only increase muscle length; they also increase muscle volume and performance.
The entire routine of stretches and exercises takes a little over 20 minutes per day to perform, but for patients who know the frustration of dealing with chronic plantar fascial pain, that will seem like a small price to pay to get rid of this nagging injury once and for all.
References
- Riddle D, Schappert S. Volume of ambulatory care visits and patterns of care for patients diagnosed with plantar fasciitis: a national study of medical doctors. Foot & Ankle Int, 2004;25:303-310.
- Hansen L, Krogh T. Ellingson T, et al. Long-term prognosis of plantar fasciitis. A 5- to 15-year follow-up study of 174 patients with ultrasound examination. Orthop J Sportsmed, 2018;6:1-9.
- Sullivan J, et al. Musculoskeletal and activity-related factors associated with plantar heel pain. Foot & Ankle Int, 2015;36:37-45.
- DiGiovani C, Kuo R, Tejwani N, et al. Isolated gastrocnemius tightness. J Bone Joint Surg, 2002;(84A):962-971.
- Pearce C, Seow D, Lau B. Correlation between gastrocnemius tightness and heel pain severity in plantar fasciitis. Foot & Ankle Int, 2021;42:76-82.
- Chimera NJ, Castro M, Manal K. Function and strength following gastrocnemius recession for isolated gastrocnemius contracture. Foot & Ankle Int, 2010;31:377-384.
- Arshad Z, Aslam A, Razzaq M, et al. Gastrocnemius release in the management of chronic plantar fasciitis: a systematic review. Foot & Ankle Int, 2022 Apr; 43(4): 568-575.
- Panid L, Bogdanis G, Terziz G, et al. Muscle architectural and functional adaptations following 12-weeks of stretching in an adolescent female athletes. Front Physiol. July 2021;12: 701338.
Click here for more information about Thomas Michaud, DC.