






Before I give you an example of a minor paradigm shift I recently experienced, (evaluation of the supraspinatus muscle), I would like to express how impressed I was with NYCC and its president, Dr. Frank Nicchi. Years ago, after learning about motion palpation from Dr. Len Faye, I introduced it to NYCC in Long Island, N.Y. I loved the Long Island campus and was saddened to see it change locations. But what a surprise it was when Dr. Nicchi escorted me around the 286-acre campus in the heart of the Finger Lakes region of upstate New York. (It was originally the Eisenhower College.)
Present-day NYCC is a modern facility, containing state-of-the-art computer labs and distance learning capabilities, a newly renovated 8,000-square-foot research building, on-campus housing, and a state-of-the-art anatomy center with its own morgue. NYCC has three off-campus chiropractic health centers, and offers participation in nearby hospital rotations. I was also impressed with the electives the college offers, such as Graston technique, sports chiropractic, practice management, pediatrics, chiropractic techniques, and geriatrics. In addition to a multipurpose athletic center, there is also a nine-hole executive golf course. Our profession is very fortunate to have NYCC.
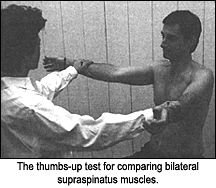
Most of the testing for supraspinatus tendinopathy is usually done with the examiner facing the patient with both arms in 90-degree abduction and in the scapular plane (30-degree horizontal adduction), with the thumbs pointing downward.1 I have always found this test to elicit more pain than the same test with the thumbs-up "full can" position, and assumed it to be a more sensitive test. But the most EMG activity of the supraspinatus, which most minimizes the synergistic infraspinatus activity, is via the thumbs-up position.
A recent study2 found that with Jobe's test (thumbs down), since the shoulder is put in a position of medial rotation, which is an impingement test position, there will be increased sensitivity, but a lack of specificity. Sensitivity means that if a patient has a supraspinatus problem, there will be a positive test result, but since there are many other shoulder areas that can be impinged in the medial rotation position (low specificity), this position will be positive in all conditions responsible for pain during medial rotation. The pain elicited is not necessarily pinpointing the supraspinatus as the problem, although it may be involved. Lack of specificity for the thumbs-down test (proportion of true negatives without the condition) therefore indicates that it is not necessarily the supraspinatus.
With all functional tests, it is also important to palpate the possible local areas that may be treated for tenderness compared to the opposite side, and after treatment, to do a functional test to determine if there is pain relief. For example, for the supraspinatus, the three most common areas involved are the insertion, the musculotendinous portion or the belly. The authors2 also thought that the test for the long head of the biceps, with the elbow extended and pushed anteriorly against resistance (Speed's test), had no diagnostic value because of very low or no specificity, due to the lever arm created by the position required by the test. Last month's article in DC3 may confirm this idea, since it was found that the biceps was much more active during elbow motion than with shoulder motion.
References
- Jobe FW, Jobe CM. Painful athletic injuries of the shoulder. Clin Orthop 1983;173:117-124.
- Leroux J-L, Thomas E, Bonnel F, Blotman F. Diagnostic value of clinical tests for shoulder impingement syndrome. Revue Du Rhumatisme (Engl Ed.), 1995;62(6):423-428.
- Hammer W. Is tenderness of the long head of the biceps important? Dynamic Chiropractic, Sept. 13, 2004: www.chiroweb.com/archives/22/19/13.html.
Warren Hammer, MS, DC, DABCO
Norwalk, Connecticut
www.warrenhammer.com
Click here for previous articles by Warren Hammer, MS, DC, DABCO.