






If it is injured, the supraspinatus will test weak, suffering from disuse atrophy or inhibited due to pain. But what if the weakness is secondary to a malfunctioning scapula, known as scapula dyskinesis (i.e., an alteration in the normal position or motion of the scapula during coupled scapulohumeral movements)?1 If the normal function of the scapula is altered, the muscles originating off the scapula, such as the rotator cuff muscles, may become dysfacilitated and test weak.
The scapula normally rotates medially and upwardly as the arm elevates. The scapula also tilts posteriorly. Posterior tilting refers to the inferior portion of the scapular shifting anteriorly, which allows the acromion to be kept away from the subacromial space containing the bursa and cuff muscles. During humeral elevation, most of the posterior tilting occurs after 90 degrees and sharply increases at the end range. With abnormal decreased posterior tilting, there may be impingement on the cuff muscles by the acromion shifting anterior-inferior. Muscle tightness in the pectoralis minor and short head of the biceps, and tightening of the pectoral fascia, can be responsible for causing anterior scapular tilting. There also may be associated weakness in lower trapezius, rhomboids and serratus anterior, resulting in scapular dyskinesis.
It was found that one of the main effects of scapular dyskinesis is a scapular that undergoes excessive protraction3 (i.e., a scapula that shifts more anterior than normal), which decreased maximum rotator cuff activation by 23 percent.4 Smith showed that maximum rotator cuff strength was related to a position of neutral scapular protraction/retraction and that if not in the neutral position, there would be decreased rotator cuff abduction strength.4,5
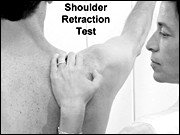 Therefore, it is apparent that the position of the scapular if abnormal will affect strength testing for the cuff muscles and especially the supraspinatus. This means that after we test the supraspinatus to find the true strength of this muscle, it is necessary to retest, making sure the scapular is in its normal retracted position. In the figure above, the examiner stabilizes the acromion with the hand and holds down the medial border of the scapula with the forearm. While maintaining this position, the supraspinatus and other cuff muscles can be tested. Even if the supraspinatus tests strong in an asymptomatic patient, retesting with the scapula in the retracted position may show increased strength and therefore represent a scapula involvement preventing maximum strength. A retracted scapula acts as a stable base for the origin of all the rotator cuff muscles.4 While the scapular muscles as well as the anterior shoulder muscles (pectoralis major and minor) may be deficient, the problem may stem from weakness in the kinetic chain affecting scapular retraction, such as core stabilization of the trunk.4 If the supraspinatus remains weak with scapular retraction, rehabilitation should be directed to the supraspinatus and other cuff muscles. I have found increased strength of the infraspinatus recently by stabilizing the scapula.
Therefore, it is apparent that the position of the scapular if abnormal will affect strength testing for the cuff muscles and especially the supraspinatus. This means that after we test the supraspinatus to find the true strength of this muscle, it is necessary to retest, making sure the scapular is in its normal retracted position. In the figure above, the examiner stabilizes the acromion with the hand and holds down the medial border of the scapula with the forearm. While maintaining this position, the supraspinatus and other cuff muscles can be tested. Even if the supraspinatus tests strong in an asymptomatic patient, retesting with the scapula in the retracted position may show increased strength and therefore represent a scapula involvement preventing maximum strength. A retracted scapula acts as a stable base for the origin of all the rotator cuff muscles.4 While the scapular muscles as well as the anterior shoulder muscles (pectoralis major and minor) may be deficient, the problem may stem from weakness in the kinetic chain affecting scapular retraction, such as core stabilization of the trunk.4 If the supraspinatus remains weak with scapular retraction, rehabilitation should be directed to the supraspinatus and other cuff muscles. I have found increased strength of the infraspinatus recently by stabilizing the scapula.
Other possible causes of scapular dyskinesis are shortened clavicles due to fractures, acromioclavicular arthrosis, and injuries resulting in acromioclavicular instability, all of which may alter scapular kinematics.
Scapular dyskinesis may be related to poor posture, such as excessive thoracic kyphosis and cervical lordosis, which may be causative of excessive scapular protraction and acromial depression resulting in impingement. With slouching or thoracic kyphosis there is less-than-normal posterior tilting of the scapular, predisposing to an impingement syndrome by narrowing of the subacromial space during shoulder elevation. A weakened rotator cuff muscle may appear and become stronger with the scapular retraction test.
References
- Kibler WB, McMullen J. Scapular dyskinesis and its relation to shoulder pain. J Amer Acad Orthop Surg 2003;11(2):142-151.
- Kibler B. Role of the scapula in the overhead throwing motion. Contemp Orthop 1991;22:525-532.
- Kebaetse M, McClure PW, Pratt NA. Thoracic position effect on shoulder range of motion, strength, and three-dimensional scapular kinematics. Arch Phys Med Rehabil 1999;80:945-950.
- Kibler WB, Sciascia A, Dome D. Evaluation of apparent and absolute supraspinatus strength in patients with shoulder injury using the scapular retraction test. Amer J Sports Med 2006;10(10):1-5.
- Smith J, Kotajarvi BR, Padgett DJ, Eischen JJ. Effect of scapular protraction and retraction on isometric shoulder elevation strength. Arch Phys Med Rehabil 2002;83:3667-370.
Click here for previous articles by Warren Hammer, MS, DC, DABCO.