






Since this case is ongoing, I've redacted the names and dates, but the other details are real. Also, I've quoted from the report most of the time, signed by two engineers, proving, I suppose, that two who are wrong cannot make something right. Both hold master's degrees in mechanical engineering. Sections in brackets are summarized for the sake of brevity.
Facts about the Accident
In the body of the report it was noted that Mr. and Mrs. McCoy (aliases) had stopped for traffic in a Plymouth Voyager. It was struck from the rear by a Ford Taurus wagon. A police report was made, and it was noted that the McCoys were wearing safety restraints. Mrs. McCoy was not injured, according to the police officer; Mr. McCoy was noted to have a "possible injury." Color photographs of the Plymouth were available for review and showed "superficial cosmetic damage which does not reflect a significant impact." A repair estimate for the Plymouth totalled $331.60. "Original color photographs" of the Ford show damage to the license plate frame. No damage estimate was available.
Summary of the Engineering Report
Parts of the report are nothing more than padding and fluff designed, I imagine, to add a veneer of credibility. I have omitted those sections/comments in the interest of brevity. I have numbered the paragraphs and sentences that follow so that I can refer to them later in my section on Rebuttal Issues. Unless in brackets, these are direct quotations. I'll reserve all comments for the Rebuttal Issues section.
- From an objective biomechanical engineering perspective, the subject traffic accident did not expose Richard McCoy, age 65, or Margaret McCoy, age 63, to profound impact or acceleration forces.
- We calculated that they each reasonably experienced an average body acceleration of 1.7 g, which potentially produced average inertial head accelerations of up to 3.4 g. Forces of this magnitude are considered minor and are comparable to forces of typical daily activity.
- We conclude that the accident was not consistent with causing physical harm. Due to their relatively advanced age and physiological conditions they may have experienced, at most, some minor transient discomfort.
- The collision analysis considered the "worst case" scenario and considered the following factors:
- [The curb weights of each vehicle.]
- [Weather conditions.]
- The extremely minor damage to each vehicle was consistent with the type of damage that occurs from an impact at very low velocity.
- Based on the location of damage to the Ford's front end, this accident appears to have involved a concentrated or point load impact. In this regard, the protruding front license frame was the primary location of contact. Because point or concentrated load impacts yield more damage and produce less acceleration than do full bumper face impacts, they are less detrimental to the occupants of each vehicle.
- The Plymouth was equipped with bumpers that are rigidly mounted to the vehicle frame; there were no absorbers to dissipate energy. As a consequence, this type of bumper typically buckles, fractures, or sustains other deformation from even low velocity impacts.
- The Ford was equipped with a bumper system which disperses impact energy through piston-type shocks ... thus reducing the amount of energy which can be transmitted to the occupant compartment.
- In low velocity impacts between an energy absorbing bumper and a rigidly mounted bumper, the vehicles exhibit up to 45% loss in kinetic acceleration energy.
- In accordance with Federal Motor Vehicle Safety Standards, all passenger vehicles manufactured after 1983 must be equipped with front and rear bumpers that can sustain barrier impacts of up to 2.5 mph without incurring structural damage.
- Based on vehicle weights, the magnitude of plastic fracture of the deformed components, and the data which has been extrapolated from empirical low velocity crash tests, we calculated that the Ford's relative closing velocity was 6.9 mph.
- We calculated that the Plymouth's impact-related forward acceleration was 55 ft/sec2, or 1.7 g. Due to the rigid body mechanics of automobiles and the variances among seat stiffness to energy absorption ratios, this acceleration may have caused an average inertial head acceleration of 3.4 g.
- Because of the relatively low speed nature of this accident, any difference between the inertial forces that each plaintiff experienced would have been insignificant.
- [In their discussion of the case, the engineers comment that, while Mr. McCoy was noted at the scene to have a possible injury, he did not seek medical care for three days.]
- [They go on to describe his cervical and thoracic complaints and the treating doctor's radiographic impressions of osteoarthritis in the cervical spine: Apparently, they reviewed medical records. They also note that Mrs. McCoy presented three days after the accident with essentially the same symptoms as Mr. McCoy and that she had a kyphotic configuration of the cervical spine on radiographic examination.]
- [The reviewers point out that both the McCoys related moving forward and then back after impact, which, the authors of this report note, imprecating with the ghost of Sir Isaac, is in direct defiance of Newtonian physics.]
- According to Newton's first law, the Plymouth would have moved forward while the occupants remained stationary with respect to the ground. About 60 msec after the impact, they would have had increased contact with the seatbacks, which provide excellent protection to the spinal column and minimize the potential for injury to the back. About 260 msec later, they may have experienced a minimal forward rebound which, if significant enough, would have been arrested by their safety restraints. Under these kinematics, the supported spine does not undergo any significant stresses or strains, and there is no feasible mechanism for a lower or middle back injury.
- Reportedly, Mrs. McCoy struck the back of her head on her headrest. Headrests play an important function in reducing the occurrence and severity of "whiplash" type injuries.
- [Regarding their calculated average inertial head acceleration of 3.4 g] A g force of this magnitude can best be understood when it is compared to those of normal daily activities. Coughing can create a force of up to 3 g; hopping from an eight-inch step can produce 4.5 g; plopping backward into a chair can produce up to 5.6 g.
- Citing the literature, but without giving specific references, the engineers note that load levels much higher can be tolerated without any adverse effects; and that empirical crash tests, performed under similar conditions with comparatively aged males and females have been conducted at speeds appreciably higher than those calculated in this accident without any injuries occurring.
Rebuttal Issues
These issues are presented as food for thought. You now have all the information I have, so I can't tell you which of these points will turn out to be particularly important. However, they may be very useful to the plaintiff attorney trying the case.
To begin with, we might ask whether either of these engineers are actually certified accident reconstructionists. It's a small point, but why not bring it up? Secondly, a glance at their CVs might demonstrate that none of their training involved crash testing or human biomechanics. Most biomechanical engineers, in fact, have no relevant training in this area. Frequently, you'll find that their dissertation explored, as an example, the viscoelastic properties of vascular surgical aortic implants in primates.
These authors have made a number of calculations, none of which were provided for us. We should ask them to supply us with all of the calculations so that we can see which equations they used and the variables they used in those equations. The reason we ask is because sometimes no calculations are actually made. In other cases, the engineer has made assumptions about velocity or other variables that are really not justified by the scant information available. As an aside, in a real accident reconstruction, it is customary to provide all of your calculations and assumptions. When they are not provided it suggests a lack of sincerity.
Here are a few other general points of criticism. Obviously, no actual vehicle inspections took place. They discussed bumper isolators on the Ford, but we don't really know whether they were damaged or even functional. They looked at "original photographs" of the Ford. Were the photos of the Plymouth photocopies? Also, did the photos include views of the bumper components? Usually they do not, despite the fact that these are some of the most important to see if you don't have the luxury of an actual vehicle inspection. Insurance claims adjustors tend to minimize the appearance of damage in these pictures. But after a car has been repaired, there is virtually nothing else to look at.
They had a damage estimate for the Plymouth, but apparently no actual repair documentation. Were there any discrepancies? This could be significant. And what about the Ford? They didn't even mention a repair estimate in their report. Sounds fishy to me.
A police report was mentioned as well. Usually, the investigating officer estimates a collision speed. It was not mentioned by our engineers in their report. Why not? Was it different from their calculation? The numbered paragraphs that follow correspond to those above.
- Notice the wording: "objective?" Please, guys, don't even say it. And how are these engineers defining "profound impact or acceleration forces?" If profound is synonymous with "very serious," the statement itself is lacking in profundity.
- Reporting average acceleration is a common method of trivializing an incident. The dangers of reporting measures of central tendency (means, medians, and mode) are illustrated by the old joke about the statistician who drowned fording a river with an average depth of three feet. In collision analysis we can look at it using the equation:
a= V/t eq.1 where a is acceleration in ft/sec,2 V is the change of velocity in ft/sec, and t is time in seconds. We know from several full scale crash tests that maximum acceleration of an occupant in a 5 mph (7.35 ft/sec) crash will occur in about 0.120 seconds. Thus, the average acceleration will be 61.3 ft/sec.2 Since 1 g is 32.2 ft/sec,2 we can divide this figure by 32.2 and get 1.9 g. However, this is the acceleration of the vehicle. The heads of occupants are known to be accelerated to two or more times that of the vehicle.1-10 Moreover, peak accelerations, in contrast to average accelerations, as high as 12-16 g,11 have been measured at the heads of human volunteers in such crash tests. And, when we speak of human injuries, it is most meaningful to report peak values rather than average values which might otherwise obscure injurious levels of acceleration. I plotted a regression curve and developed a crude regression equation based on real crash data, Figure 1 [west graph].12 The graph suggests that the engineers' estimate (in the present report) of an average of 3.4 g at the head may be quite low.
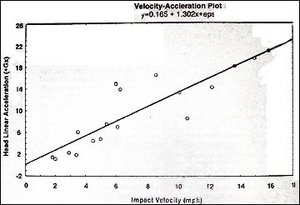
Figure 1: Regression curve of velocity and head linear acceleration. From reference 12.
And what about that comment about "comparable to normal everyday activity?" Well maybe, if you happen to be a test pilot. Say you wanted to calculate the average acceleration of a jet aircraft launched from an aircraft carrier deck. Assuming an elapsed time of 2.5 seconds at an elapsed speed of 200 mph (I'm making these numbers up), the acceleration would be a=294 ft/sec/2.5 or 117.6 ft/sec2 (3.7 g).
- This conclusion is, of course, made without examining the people complaining of injuries and without any medical training or real life clinical experience. See comments below under General Issues.
- I was trained, as an accident reconstructionist at Northwestern University, to provide a range of values for speeds and other parameters. This "worst case" method used by these authors is commonly employed in this genre of report, I suspect, because an honest portrayal of facts would not be propitious for the client. Imagine the difference between saying that the range of values for collision speed was 2.1-6.9 mph, and simply saying it was 6.9 mph. In the former, one immediately recognizes some degree of imprecision, whereas the latter invokes a bit more certitude. And why 6.9 mph? Since it is admittedly only an estimate, why not simply report 7 mph? Does 6.9 sound a more accurate? How would you estimate the balance in your bank account? To the nearest cent?
- If the curb weights were used, the authors must have used either a kinetic energy equation or conservation of momentum equation. Again, it would be nice to see their work. However, one wonders how they arrived at the necessary velocity value for either equation. In other words, to determine the acceleration of the occupants, you need to determine the delta V of the Plymouth. To do this you start with an impact velocity of the Ford. That usually comes from vehicle dynamics equations. But there is nothing to help us in that regard -- no skid marks and not enough damage to use a barrier equivalent velocity equation -- so 6.9 mph has appeared. From what I can gather, it was estimated through some sort of engineering Gestalt or formulae containing secret Ouija board constants. There are no known means of making the "calculation" for impact velocity given the information they claimed to have. Thus, all other calculations are subject to the same uncertainty.
- Not important.
- Notice the wording again: "extremely minor" and "very low."
- Very interesting, as Henry Kissinger would say, particularly if it has the added virtue of being true. This may be a moot issue though, because they told us they don't know enough about the damage to verify this anyway.
- This is not likely to be true. As the authors themselves point out later, energy attenuating bumper systems are a requirement on all late model passenger vehicles. They don't have to be bumper isolators like the Ford had, but some type will have been in place: polyurethane foam or rigid corrugated one-shots, for example. And, this brings up an important point. If both cars had 5 mph rated bumpers, theoretically, they could have withstood a crash of 10 mph without sustaining any significant damage.
- This statement is made to suggest that these isolators absorbed a good deal of the energy before it could be transmitted to the occupants. However, studies looking at the effect of isolators on rear impact collisions have not borne this out.14 Moreover, they were designed, and later mandated, to reduce the threshold of damage to automobiles while preserving safety features such as tail lights and exhaust pipes; not to reduce occupant loads. This is a very common, albeit specious, defense argument.
- This is not a figure I am familiar with, but appears to conflict with tests that have been conducted on these bumper systems. I'd ask for their source of information.
- Yes, and in some years, the requirement has been 5 mph. Their point here is obscure. They don't even mention the specific ratings of the bumpers of the involved vehicles. I wonder if they checked.
- Here's that Gestalt part. They didn't examine the plastic damage or deformed components. Eye of newt, hair of toad ... Sounds impressive though.
- They are probably using a delta V of about 4.5 mph to get this figure, which is probably about right if we are comfortable with the 6.9 mph impact figure. But remember, that's a dubious estimation of impact velocity. Most reputable accident reconstructionists wouldn't hazard more than a qualified guess about velocity of impact with such scant data.
- Their lack of clinical experience and lack of familiarity with the literature is apparent here. As all clinicians know, a wide variance in injury potential exists in occupants of the same vehicle. Part of this variance can be explained by the large difference in occupant position, with the so-called out-of-position occupant being exposed to much higher inertial loading than one seated normally.5,14-18 Other sources of variance have been observed by researchers noting a difference in occupant acceleration between preparedness and surprise.1 Moreover, poor clinical outcome has recently been associated with a lack of preparedness.19,20 Finally, if perhaps a bit punctilious, I make it a habit not to use the terms "plaintiff" and "defendant." Nor do I use the word "alleged." These are legal terms and tend to blur the distinction between the duties and goals of doctors and attorneys.
- This is a twist of the old "delayed onset" stratagem. In Mr. McCoy's case, there apparently was initial discomfort, but he earns credibility demerits, nevertheless, for his delay in seeking care. Whether this is relevant to the case or not, the issue clearly does not seem to be within the purview of our tag team of mechanical engineers.
- Now it is Mrs. McCoy who's attacked with the delayed onset innuendo. But now, in discussing radiographic findings, these guys are definitely playing doctor. In any case, a kyphotic angulation can definitely suggest significant injury in such an accident, especially in a 63-year- old spine.
- Here, the authors seem to be attempting to show that the McCoys have confected a story that is simply not feasible and, thus, they've been caught in a lie. It suggests that the analysis has again gone astray of its stated goals of an "objective biomechanical engineering" assessment. In my research, I've found that patients invariably do report the mechanism of injury as a 'first forward, then back' phenomenon. I imagine that is because the accident happens in less than a third of a second and they are not even aware of the initial motion. A minor point in either case.
- "Increased contact," is a nice euphemism, and all of this is merely speculative; partially true if the occupants are seated in the ideal position. However, the seatbacks do not provide excellent protection. It's known that back injuries occur in about 35% or more of rear impact injuries,21-26 although the exact mechanism of this is not known. Shoulder harnesses are widely known to increase the potential for neck injury in these low speed rear impact collisions.27-34 This paragraph is entirely inaccurate to the point of being silly.
- Again, note the wording, "reportedly." Would it be unlikely? In any case, their version of reality differs significantly with the literature. Yes, head restraints were 'designed' to play an important role. Sadly, to date, their ability to prevent or mitigate whiplash injury has been a dismal failure. While some studies have shown that they reduce injuries by 11-24%,28 others have suggested that they actually increase the potential for injury.5 Recently, the Insurance Institute for Highway Safety rated only 3% of modern head restraints as good.35 Many restraints will drop to their low position when hit by the occupant's head and then act as a fulcrum, resulting in measurably higher loads than seats without any restraints.36
- I haven't seen the literature concerning coughing, but I would bet that the g forces were not measured in the same way as in rear impact accident crash tests. Certainly, we don't see a lot of sneezing injuries in clinical practice. Hopping from a curb produces g force impulses measurable chiefly through the lower extremity, not the cervical spine in the +Gx direction. Moreover, these spikes of acceleration have very brief durations, as do those measured in chair plopping,37 a magnitude less than those measured in volunteers exposed to rear impact crash tests.
More specious mumbo jumbo. These comparisons are devilishly cleaver subterfuge, but thoroughly unscientific and clearly sophistic -- a sort of scientific legerdemain that wins juries every time unless exposed for what it is: the sound of the one eye winking.
- To begin with, we have questioned their calculated load levels. I don't know of any published studies using 60 year old volunteers in crash tests. I had to laugh when I read this part; I'd certainly like to see that research. Of all of the published crash testing, I am aware of only one in which some of the volunteers were women.38 One of them was in her 50s at the time, and may be the oldest to participate in such studies. However, that crash testing produced delta Vs of only 5 mph at maximum; minor transient discomfort was reported by some volunteers. So the load levels were at most marginally in excess of what the McCoys were exposed to.
It's important to remember that these laboratory tests are highly controlled and volunteers are rarely out of position and never fully unprepared for the impact. Moreover, most of the tests have been conducted by research labs whose primary clients are insurance companies and defense lawyers. I've had direct experience with some of these.
Finally, one of the truly outstanding studies did show that a delta V of 5 mph was the threshold for cervical soft tissue injury; and that was in adult healthy male volunteers.39 In a real world hexogenarian motorist, with degenerative disease in the neck, who is, perhaps, caught unaware, this threshold is likely to be much lower, particularly in women. A 6.9 mph impact would produce a delta V of 3.5-4.5 mph. So it would seem that an injury in this case is far from implausible.
General Issues
I have no doubt that the defense law firm that hired these engineers would be delighted to believe even a portion of this report. They will, in any case, proceed as though it were the Gospel. (Quotations from Sir Isaac Newton suggest that it is at least close!) On the other side of the fence, any plaintiff attorneys worth their salt will realize that the most important variables are the patients themselves. Forget, for the moment whether a couple of bridge builders can predict whether the patients should have, would have, or could have been injured. The burning question is: are they really injured or not? How do we know? This is the purview and the exclusive domain of doctors. And, while engineers and accident reconstructionists make occasional misadventurous forays into this area, they are decidedly unqualified poseurs and woefully inept. And, in my opinion, they should be reprimanded whenever they try to play doctor.
At this deepest level, you as a doctor, whether treating or examining, will decide, based on your training and experience, whether bona fide injuries have actually occurred or not. That is the only real issue. Then you can classify the patient based on published grading schemes.
Think about it this way: Would it really make any difference if a panel of boxing experts got together after the last Tyson fight and decided that Tyson should have won by KO in the 4th round? No. Tyson lost, period: That's all that really matters. And all of this wrangling about delta V and g forces is really a pointless and naive exercise anyway. The very fact that some occupants are injured while others are not in the same accident should be evidence enough that precise knowledge of these crash parameters is insufficient information to allow us to predict who will be injured and to what degree. Instead, the very complex dynamic interplay between vehicles and occupants is only poorly understood, yet is, in conjunction with the overflowing pastiche of human variables, the key to understanding the phenomenon of whiplash. Thus, we have rendered the accident reconstructionist an unnecessary novelty in LOSRIC since, on the one hand, he/she cannot predict the actual collision velocities with any meaningful precision and, on the other hand, because knowing the precise impact velocity value would be meaningless anyway, since we do not have any satisfying way of associating collision velocities (or acceleration) and human pathology.
Finally, we must always remember that about 2 million injuries occur each year in the U.S. (12-page 7) and the majority are in low speed rear impact types occurring at collision speeds of between 6 mph and 12 mph40 where, incidentally, other studies have shown that vehicle damage thresholds are just being reached.8,11,41,42 Intuitively then, we would expect that, in most cases, damage would be minimal. Thus, to predict that injuries are not possible based on minor vehicle damage alone, we might be wrong as much as 50% or more of the time. But then, it's easy to say beneath the whisper of the eye winking.
References
- Severy DM, Mathewson JH, Bechtol CO: Controlled automobile rear-end collisions, an investigation of related engineering and mechanical phenomenon. Can Services Med J 11:727-758, 1955.
- Severy DM, Mathewson JH: Automobile barrier and rear-end collision performance. Paper presented at the Society of Automotive Engineers summer meeting, Atlantic City, NJ, June 8-13, 1958.
- Severy DM, Mathewson JH, Bechtol CO: Controlled automobile rear-end collisions -- an investigation of related engineering and medical phenomena. In Medical Aspects of Traffic Accidents, Proceedings of the Montreal Conference, 1955, pp 152-184.
- Navin FPD, Romilly DP: An investigation into vehicle and occupant response subjected to low-speed rear impacts. Proceedings of the Multidisciplinary Road Safety Conference VI, Fredericton, New Brunswick, June 5-7, 1989.
- Romilly DP, Thomson RW, Navin FPD, Macnabb MJ: Low speed rear impacts and the elastic properties of automobiles. Proceedings: 12th International Conference of Experimental Safety Vehicles, Gothenburg, 1-14, May/June, 1989.
- Thomson RW, Romilly DP, Navin FPD, Macnabb MJ: Energy attenuation within the vehicle during low speed collisions. Report to Transport Canada, University of British Columbia, Aug, 1989.
- Thomson RW, Romilly DP, Navin FPD, Macnabb MJ: Dynamic requirements of automobile seat backs. SAE Tech Paper Series 930349, Detroit, 193-198, Mar, 1993.
- Bailey MN, King DJ, Romilly DP, Thomson RW: Characterization of automobile bumper components for low speed impacts. Proceedings: Canadian Multidisciplinary Road Safety Conference VII, Vancouver, British Columbia, 190-203, Jun, 1991.
- Thomson RW, Romilly DP: Simulation of bumpers during low speed impacts. Proceedings: Canadian Multidisciplinary Road Safety Conference VIII, Saskatoon, Saskatchewan, 237-247, Jun, 1993.
- Emori RI, Horiguchi J: Whiplash in low speed vehicle collisions. SAE Paper 900542, Detroit, 103-108, 1990.
- West DH, Gough JP, Harper TK: Low speed collision testing using human subjects. Accid Reconstr J 5(3):22-26, 1993.
- Croft AC: Whiplash: the Masters' Program. Module 1. Whiplash: Advanced Topics. San Diego, Spine Research Institute of San Diego, 1996, p17.
- Bailey MN, Wong BC, Lawrence JM: Data and methods for estimating the severity of minor impacts. SAE Tech Paper Series 950352 1339-174, 1995.
- Hu AA, Bean SP, Zimmerman RM: Response of belted dummy and cadaver to rear impact. SAE 770929, in Proceedings of the Twenty-First Stapp Car Crash Conference, Society of Automobile Engineers, 587-635, 1977.
- Berton RJ: Whiplash: tests of the influential variables. SAE 680080, Automotive Engineering Congress, Detroit, MI, Jan, 1968.
- Foret-Bruno JY, Tarriere C, LeCoz JY, et al.: Risk of cervical lesions in real-world and simulated collisions. 34th AAAM Conference Proceedings, Scottsdale, AZ, p373, Oct, 1990.
- Olsson I, Bunketorp O: An in-depth study of neck injuries in rear end collisions. IRCOBI, p269, Sep, 1990.
- Severy DM, Brink HM, Baird JD: Preliminary findings of head support designs. SAE 670921 in Proceedings of the 11th Stapp Car Crash Conference, 1967.
- Sturzenegger M, Di Stefano G, Radanov B, Schnidrig A: Presenting symptoms and signs after whiplash injury: the influence of accident mechanisms. Neurology 44(4):668-693, 1994.
- Ryan GA, Taylor GW, Moore VM, Dolinis J: Neck strain in car occupants: injury status after 6 months and crash-related factors. Injury 25(8):533-537, 1994.
- Foreman SM, Croft AC: Whiplash Injuries: The Cervical Acceleration/Deceleration Syndrome. Baltimore, Williams & Wilkins Co., 1988, p 293.
- Braaf MM, Rosner S: Symptomatology and treatment of injuries of the neck. NY State J Med 55:237-242, 1955.
- Hohl M: Soft tissue injuries of the neck in automobile accidents: factors influencing prognosis. J Bone Joint Surg 56A(8):1675-1682, 1974.
- Bring G, Westman G: Chronic posttraumatic syndrome after whiplash injury: a pilot study of 22 patients. Scan J Prim Health Care 9:135-141, 1991.
- Gargan MF, Bannister GC: The rate of recovery following whiplash injury. Eur Spine J 3:162-164, 1994.
- Magn£sson T: Extracervical symptoms after whiplash trauma. Cephalalgia 14(3):223-227, 1994.
- Dunn EJ, Blazar S: Soft-Tissue injuries of the lower cervical spine. Instructional Course Lectures, American Academy Orthopaedic Surgeons, Vol XXXVI, 499-512, 1987.
- Nygren A: Injuries to car occupants--some aspects of interior safety of cars. Acta Oto-Laryngologica (Suppl #394), 1984.
- Ommaya A, Backaitis S, Fan W, Partyka S: Automotive neck injuries. Ninth Internatl Technical Conference on Experimental Safety Vehicles, US Department of Transportation, National Highway Traffic Safety Administration, Kyoto Japan, Nov 1-4, 1982, pp 274-278.
- Deans GT, Magalliard JN, Kerr M, Rutherford WH: Neck sprain--a major cause of disability following car accidents. Injury 18:10-12, 1987.
- Yoganandan N, Haffner M, Maiman DJ, et al.: Epidemiology and injury biomechanics of motor vehicle related trauma to the human spine. SAE 892438, in Proceedings of the 33rd Stapp Car Crash Conference, Detroit, MI, Society of Automotive Engineers, 223-242, 1989.
- Balla JI: Report to the Motor Accidents Board of Victoria on whiplash injuries. In (Chapter 10) Headache and cervical disorders. In Hopkins A, ed., Headache: Problems in Diagnosis and Management. London, Saunders, 1988, pp256-269.
- Juhl M, Seerup KK: Cervical spine injuries: epidemiological investigation. Medical and social consequences. (MOVE) 49-57, 1981.
- HUK-Verband: Sicherheit im auto: das unfallgeschehen und seine Folgen HUK-Verband, Muchen, 34-35, 1975. 35. Head restraints with good geometry can reduce neck injuries. Accid Reconstr J 7(5):53-54, 1995.
- Onon K, Kanno M: Influence of the physical parameters on the risk to neck injuries in low impact speed rear-end collisions. Accid Anal Prev 28(4):493-499, 1996.
- Allen ME, Weir-Jones I, Motiuk DR, et al.: Acceleration perturbations of daily living: a comparison to 'whiplash.' Spine 19(11):1285-1290, 1994.
- Szabo TJ, Welcher JB, Anderson RD, et al.: Human occupant kinematic response to low speed rear-end impacts. SAE Tech Paper Series 940532 23-35, 1994.
- McConnell WE, Howard RP, Guzman HM, et al.: Analysis of human test subject kinematic responses to low velocity rear end impacts. SAE Tech Paper Series 930889 21-30, 1993.
- Olsson I, Bunketorp O, Carlsson G, et al.: An in-depth study of neck injuries in rear end collisions. 1990 International IRCOBI Conference, Bron, Lyon, France, September 12-14, 1-15, 1990.
- Wolley RL, Strother CE, James MB: Rear stiffness coefficients derived from barrier test data. SAE 910120, 1991. (chk. MOVE)
- Szabo TJ, Welcher J: Dynamics of low speed crash tests with energy absorbing bumpers. SA 41. E Tech Paper Series 921573, 1-9, 1992.
Arthur Croft, DC, M.Sc., FACO
San Diego, California
E-mail:
Click here for previous articles by Arthur Croft, DC, MS, MPH, FACO.