





As mentioned in part 2 of this cervical series, the medulla oblongata extends into the lower foramen magnum of the occiput and the ligamentous ring that connects with the atlas. The inferior olivary neurons are sensitive to pressure from occipital-atlanto (O/A) position. One of the many functions of the inferior olivary bodies is to allow "oscillation" back and forth for lateral shifting at the O/A articulation, which then affects the entire musculoskeletal system.
Side-Dominant Muscle Patterns
The diagram included in this article represents the position of the occipital bone to the atlas and the relationship with side-dominate groups or chains of muscle patterns. Jason Masek, PT, who practices at the Postural Restoration Clinic in Lincoln, Neb., created he diagram based on the writing of Philip E. Greenman, DO, from his book, Principles of Manual Medicine, 2nd Edition.
In my previous articles, I have mentioned that most of us love right mid-stance, or standing predominately on the right leg, as a common human gait pattern and position. Chains of muscles that are dominate include ones from the left lower extremity, the right upper chest wall and right neck, all of which drive musculoskeletal position.9
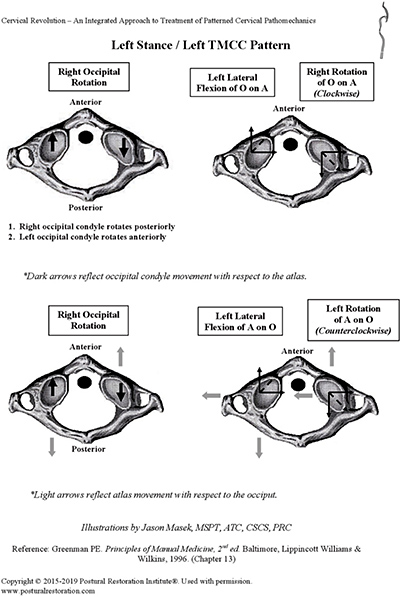 O/A joint alignment and balance involves more than 20 pairs of muscles that connect the skull, spine and shoulder girdle,1 including the dominate right temporal mandibular cervical chain (R TMCC) of muscles. The R TMCC pattern drives the atlas into mild right relative rotation as the occipital bone is simultaneously turning to the left with C2, C3 and C4 below turning left as well. The occipital bone turns left as the atlas rotates slightly right via the R TMCC. The occipital bone and entire cranium are both affected by cervical position as the right condyle of the occipital bone is put into a position of flexion over the right fossa of the atlas and the left condyle of the occipital bone is put into extension over the left fossa of the atlas. The entire cranium is affected by the position of the O/A joint including positional strain into the sphenoid and temporal bones known in osteopathic terms as cranial left side-bending physiologic position.8
O/A joint alignment and balance involves more than 20 pairs of muscles that connect the skull, spine and shoulder girdle,1 including the dominate right temporal mandibular cervical chain (R TMCC) of muscles. The R TMCC pattern drives the atlas into mild right relative rotation as the occipital bone is simultaneously turning to the left with C2, C3 and C4 below turning left as well. The occipital bone turns left as the atlas rotates slightly right via the R TMCC. The occipital bone and entire cranium are both affected by cervical position as the right condyle of the occipital bone is put into a position of flexion over the right fossa of the atlas and the left condyle of the occipital bone is put into extension over the left fossa of the atlas. The entire cranium is affected by the position of the O/A joint including positional strain into the sphenoid and temporal bones known in osteopathic terms as cranial left side-bending physiologic position.8
As right stance phase of gate is correlating with the R TMCC pattern, the right side of the atlas is actually pushing up and under the occipital bone as the right portion of the occiput is slightly lateral flexing down toward the right transverse process of the atlas.3 This is all occurring as the upper cervical spine is laterally flexing to the left with a right shoulder that is lower than the left. This postural presentation can often be seen in our patients as they stand on the right leg with a right shoulder down and head tilted to left.
Revisiting Lateralization
A vital concept to remember from parts 1 and 2 of this series is how lateralization occurs or is driven at the cervical spine. The position of the O/A joint can be driven from top down via occlusion, vestibular-ocular reflex, vision alone, trauma, toxins and emotions. However, it can also be driven from bottom up via an ankle or foot injury, knee or hip pain, breathing dysfunction (remember, the diaphragm attaches to the lumbar spine and ribs) and especially by relying on end-range position for a sense of stability in gait or standing on the right side.4 An overreliance on lateralization via end-range position for a sense of stability will create joint pathology over time, as well as compensatory neurologic patterns for movement.
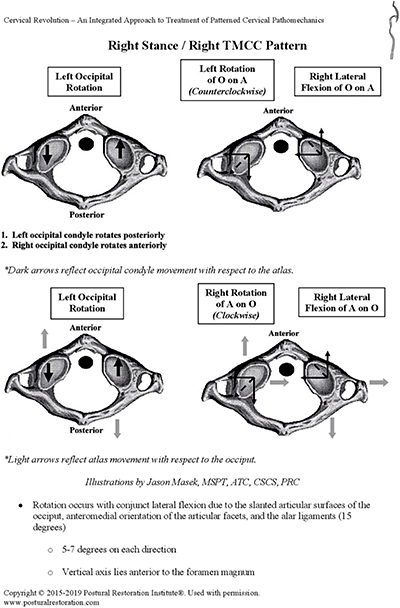 The goal is to enable an O/A joint transition from a R TMCC pattern to a L TMCC pattern as illustrated by the schematic drawing.3 Brain stem pressure can be relieved by a dynamic oscillatory position right to left side with alternation depending on which leg the patient has authentic mid-stance. Authentic just means they can turn an acetabulum over a femur and that a femur can adduct during mid-stance phase of gait, which can be determined by objective testing via an adduction drop test.9
The goal is to enable an O/A joint transition from a R TMCC pattern to a L TMCC pattern as illustrated by the schematic drawing.3 Brain stem pressure can be relieved by a dynamic oscillatory position right to left side with alternation depending on which leg the patient has authentic mid-stance. Authentic just means they can turn an acetabulum over a femur and that a femur can adduct during mid-stance phase of gait, which can be determined by objective testing via an adduction drop test.9
Most patients do not authentically stand on the left leg and as a result, cannot rotate an atlas to the left underneath an occipital bone that is simultaneously turning to the right as the upper cervical spine turns to the right and is able to laterally flex on the right!5-6 The key is learning how to inhibit the R TMCC as a result of facilitating the L TMCC for the purpose of creating a "neutral' neck that is able to rest, revolve and transition right to left side without causing undo pressure on the brain stem or creating cranial strain patterns as a result of overreliance on one side of the occipital-atlanto articulation.
Author's Note: This series will conclude next issue with a discussion of functional examination of the cervical spine.
References
- Postural Restoration Institute. Cervical Revolution Course Manual, page 5.
- Postural, Op. Cit., page 8.
- Postural, Op. Cit., pages 26-27.
- Postural, Op. Cit., page 53.
- Postural, Op. Cit., page 18.
- Neumann D. Kinesiology of the Musculoskeletal System, 2nd Edition. Mosby, 2010:341.
- Greenman PE. Greenman's Principles of Manual Medicine, 2nd Edition. Williams & Wilkins, 1996:175-177.
- James GA, Strokon JG. Cranial strains and malocclusion. Int J Orthodontics, 2006;17(3):35-39.
- George R. "Unlocking the Secrets of the Pelvis." Dynamic Chiropractic: Part 1: Aug. 15, 2013; Part 2: Oct. 1, 2013; Part 3: Dec. 1, 2013; Part 4: Jan. 15, 2014. Also: "Breathe Well and Breathe Often": Part 1: June 17, 2012; Part 2: July 15, 2012; Part 3: Sept. 9, 2012,;Part 4: Oct. 7, 2012.
- Sills F. Craniosacral Biodynamics, Volume Two: The primal Midline and Organization of the Body. North Atlantic Books, 2003:27-34.
- Postural, Op. Cit., pages 13-14.
Dr. Robert "Skip" George practices in La Jolla, Calif., where he integrates chiropractic, rehabilitation and sports performance training. He is a certified Functional Movement Screen instructor and has lectured nationally on subjects related to the chiropractic profession. He can be contacted with questions and comments at
![]() .
.