






Obviously, there are a lot of things wrong with this. What makes for good business does not necessarily make for good chiropractic. These consultants, who like most other chiropractors would like themselves seen as portal of entry and even primary care providers, do not pay much attention to details. You know, little things -- like taking a history, performing an examination, and ruling out contraindications prior to adjusting the spine. At state conventions, all that doctor stuff plays second fiddle to the solitary goal of producing audibles loud enough to hypnotize an adoring crowd amidst the din and cacophony of the exhibitor area.
A chiropractic student, having observed this same phenomenon at technique seminars, launches a remark into cyberspace: "It is amazing to me that when chiropractors go to a seminar and ask one another to give them an adjustment, it only takes a minute or two, but if you do this with a patient then you are considered irresponsible. Where is the logic here?" Dr. Badanes answers: "Apparently, no one (really) takes VS and subluxation less seriously than chiropractors themselves ... When you treat a person, whether they are a chiropractor, baker, Indian chief, or your mother, at a party, seminar, or in a restaurant bathroom, it is a bad practice to assume anything other than that they are your patient at those times."
But let us not dwell upon the undoctorly conduct of these convention doctors, for that is not my main point. Rather, let us fast-forward to a matter of pure technique: the style these doctors tend to use. Neither of the two chiropractic colleges where I have taught allowed low back moves such as these. The patient's upper leg is draped over the edge of the table and used as a crank to turn the low back, while the doctor simultaneously propels the shoulder up and away, or even pins it square to the table. There may not even be a contact hand somewhere on the low back or sacroiliac area.
This rather dramatic counter-rotation of the shoulder and pelvic girdles, the so-called "million dollar roll" (so named because doctors who employ it become millionaires?), although generally relegated to the dinosaur department in technique classes, public discussion, and probable most technique seminars, is clearly alive and well on the convention floor. Judging from the appreciative swooning of the observers, and the dazed expression of gratitude that generally adorns the subjects face as he staggers away from the table ("Thanks doc, I really needed that"), I would suspect that the millon dollar roll is also alive and well in many chiropractic offices around the country.
"The most dangerous technique in spinal manipulation is excessive rotation of the spinal column," writes a famous doctor. Perhaps, but even when a given procedure is "the most dangerous" relative to others, it does not follow that it is dangerous in the absolute, any more than saying "the most common color of Edsels is white" means there must be lots of white Edsels rolling around. Although I must remain agnostic on the relative danger of rotational lumbar moves, never having seen data one way or the other, I would be very surprised were they found to be dangerous. If indeed they were, the daily carnage in chiropractic offices around the country would have surfaced by now, and possibly even put an end to the profession.
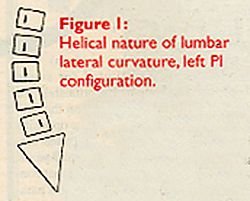
There is good reason to believe that a rotational vector in lumbar side posture adjustments may not only be safe, but indicated insofar as it addresses the helical component of the overall lumbopelvic distortion. Hugh Logan's observation1 that when the sacral base subluxates inferiorly, the lumbar spine assumes a lateral curvature convex on the ipsilateral side, has been confirmed many times. Johnston2 pointed out from a theoretical point of view that the lumbar adaptation would take the form of a spiral, while Friberg3 confirmed this helical nature of the lumbar lateral curvature through quantitative radiographic analysis. In Figure 1, although the lower spinous processes are to the left of the central ray of the x-ray, each spinous process is to the right of the spinous process of the segment below.
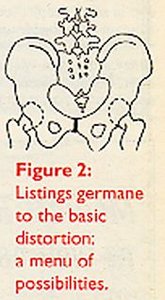
The inferiority of the sacrum is not a stand-alone finding. The entire suite of positional derangements is seen in Figure 2, which illustrates an AI sacrum left, SAR, PI-IN ilium left, AS-EX ilium right, and multiple lumbar segmental misalignments of the PRI-m persuasion. Although a strict chiropractic segmentalist would have to find a way to decide which of these listings is primary, a chiropractic structuralist4 might see the entire set of osseous positional derangements as the subluxation: a right lumbopelvic basic distortion in Logan's sense. The structuralist could also detect yet another listing: a multisegmental Y-axis helical distortion. If we regard the adjustment is segmentally specific, then by comparison the helical component of the distortion is addressed by a vectored manipulation.
Patients, while neither theoreticians nor radiometrically inclined, are intuitively aware of this helical twist in their subluxated lumbopelvic spines, at least judging from their propensity to self-manipulate it. Once in a while, patients will ask me if it is ok to twist their own backs and make popping noises. Before I furiously denounce them for being reckless with their own spine, or even for practicing chiropractic without a license, I do at least ask to be shown how it is done. Sitting on my table, the patient may lean backwards and drag their left knee across the right, keeping the left shoulder planted near the table: or maybe the patient stands up with their hands clasped near the sternum, and suddenly swings their elbows to the left while jerking the flexed left knee up and away to the right. If my descriptions are hard to visualize, just think of Chubby Checker (or anyone else) doing the twist, either supine or in the weightbearing position. By his own description, the dance requires that you "put out a cigarette with both feet and wipe your bottom with a towel."
Figure 3. Chubby Checker and friend self-manipulating, doing a bilateral weight bearing lumbar-roll.
Although Chubby Checker remains a bilateral twister, the typical patient will tell you that they generally perform their self-manipulation maneuvers in one direction only, or at least only one direction produces pops and affords relief. Which direction? Turning toward the side of their left PI-IN ilium, of course. In the standing position, friction of the patient's feet with the floor keeps the pelvic girdle relatively stationary, while the patient rotates their left shoulder girdle posteriorly on the left. Swinging their flexed left knee to the right would accentuate the effect.
The chiropractor, adjusting the left PI-IN ilium, would exert some degree of posterior pressure on the left shoulder, while thrusting the pelvic girdle anteriorly on the left. A moment's reflection will confirm that the patient and the chiropractor achieve the same relative opposed rotation of the shoulder and pelvic girdles. The doctor emphasizes an anterior thrust on the left pelvic girdle, while the patient emphasizes a posterior tug on the left shoulder girdle. I point this out not to encourage self-manipulation, but only to draw out the mechanical, diagnostic significance of the vectors that patients use in their instinctive attempt to unwind the helical component of their lumbopelvic postural distortion.
In my practice, I have developed this observation into an orthopedic sign. The standing patient is asked to clasp the hands at the waist and then rotate the torso to the end point of motion, first to the left and then to the right. One direction (toward the PI side) will subjectively feel more comfortable to the patient or exhibit less strain at the end point than the other. The patient will explain that rotation to the less favored side puts greater strain on the foot, knee, low back, and ribcage, or just feels "yucky."
The famous doctor continues: "We wouldn't want to be associated with a doctor who lumbar-rolls a patient on both sides." Although excommunication seems too harsh a sentence for the aficionado of the bilateral lumbar roll, given the lack of outcomes-based evidence on the matter, it remains likely that one direction of thrust unwinds the helical component of the patient's lumbar distortion, whereas the other direction aggravates it. I continue to be amazed by how shortsightedly some chiropractors would make pariahs out of brethren whose moves they happen to dislike, even though they have stood the test of time (e.g., rotary cervical moves and lumbar rolls), thus providing ammunition to outside detractors. (Once I found a new patient recruitment leaflet in the meat section of a local supermarket, produced by a fellow chiropractor whom I knew well, explaining how she uses safe and effective treatment methods, unlike those other chiropractors who adjust the spine using "violent, sudden, dangerous twists and jerks." Nice.)
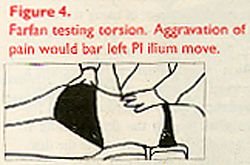
Although I am obviously making a case for a limited version of the lumbar roll, it would seem prudent, ceteris paribus, to stick to one side for most patients. Medical manipulator Harry Farfan tested lumbopelvic torsion bilaterally prior to manipulating, counter-rotating the shoulder girdle and pelvic girdle of the prone patient in an opposed manner as an orthopedic test, thus determining the preferred line of drive. Chiropractors generally perform this type of test with the patient in side posture; we simply call it setting up on the patient, or testing the adjustment prior to thrusting.
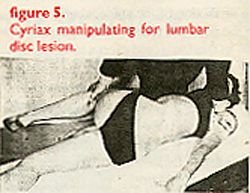
Another medical manipulator, James Cyriax, advocated highly rotated lumbar manipulation ("Applying a rotation strain is a very effective way of securing reduction at a low lumbar level") as a treatment for lumbar disc herniation, and often performed it with the patient under anesthesia -- sometimes using an assistant to increase the leverage. He believed that twisting or flexion of the spine would tighten up the posterior longitudinal ligament, so that its tension would exert a posteroanterior (centripetal) force upon the bulging annular fibers and nucleus pulposus. Chiropractor James Cox has also invoked spinal flexion as a parallel strategy to tighten up the posterior longitudinal ligament, and for the same purpose.5
How dangerous is this rotation? Farfan,6 who found that he could herniate a cadaveric lumbar disc using a combination of compression and rotation, is often invoked to support this prohibition of rotation. Nevertheless, he found that the facets would have to fracture before he could produce enough intersegmental rotation to herniate a disc, both in normal and degenerated spines. Furthermore, the pattern of disc herniation he achieved (laminar separation) did not resemble the typical radial fissures seen in real patients. Whatever clinical conclusions Farfan drew from his own work as to manipulative strategies, Cassidy et al.7 used the same data to defend the safety of sensible rotational vectors in side-posture lumbar manipulation.
One of the most peculiar phenomena I have observed in chiropractic is contempt for the practice of using rotational pre-stress or lines of drive in adjusting the spine, including the lumbopelvic area. Rotation in some quarters has become a code word for some sort of deliberately misanthropic and dangerous hatred for patients, as though the doctor using it were actually trying to herniate the disc. Sure, a "million dollar roll" does seem a bit much ... but would you believe a $50 roll, on one side only, maybe using a contact hand?
References
- HB. Textbook of Logan Basic Methods. St. Louis, Missouri. (Logan VF, Murray FM eds.)
- LC. The paradox of the functional spine. Journal of the Canadian Chiropractic Association 1966, June/July, 7-10.
- O. Leg length inequality and low back pain. Clinical Biomechanics 1987; 2:211-219.
- MJ. The structural approach to chiropractic: from Willard Carver to present practice. Chiropractic History 1981; 1 (1):25-29.
- JM. Low Back Pain, Mechanism, Diagnosis & Treatment. 4th ed. Baltimore, MD; Williams & Wilkins, 1985.
- HF. Mechanical Disorders of the Low Back. Philadelphia; Lea & Febiger, 1973.
- Cassidy JD, Thiel HW, Kirkaldy-Willis WH. Side posture manipulation for lumbar intervertebral disk herniation. JMPT 1993;16:96-103.
Robert Cooperstein, MA, DC
Faculty, Palmer West
San Jose, California
E-mail:
Click here for previous articles by Robert Cooperstein, MA, DC.