






The anterior cruciate ligament is a powerful stabilizer of the knee, possessing two different bundles (Fig. 1) that help stabilize the knee against anterior shear force, valgus collapse and excessive internal tibial rotation. Despite its overall strength, the ACL is extremely injury prone, with nearly one in 25 athletes tearing their anterior cruciate ligament annually.1
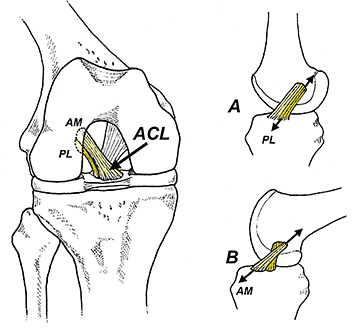 FIG 1 The anterior cruciate ligament (ACL) is divided into anteromedial (AM) and posterolateral bundles (PL). The posterolateral bundle is under peak tension when the knee is extended (A), while the anteromedial bundle is under peak tension when the knee is fl exed between 45° and 60° (B).
Given the high prevalence of this injury and the less-than-stellar outcomes following surgical reconstruction, sports medicine experts must identify athletes at risk for tearing their ACL so prophylactic exercise interventions can be performed preseason.
FIG 1 The anterior cruciate ligament (ACL) is divided into anteromedial (AM) and posterolateral bundles (PL). The posterolateral bundle is under peak tension when the knee is extended (A), while the anteromedial bundle is under peak tension when the knee is fl exed between 45° and 60° (B).
Given the high prevalence of this injury and the less-than-stellar outcomes following surgical reconstruction, sports medicine experts must identify athletes at risk for tearing their ACL so prophylactic exercise interventions can be performed preseason.
Hip Strength and Injury Risk
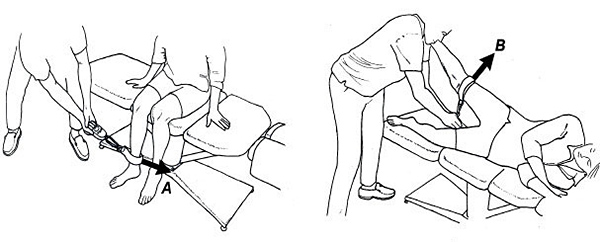
In 2016, researchers from Iran proved you could predict which athletes would tear their ACL by measuring hip strength with a dynamometer.4 Ideally, the athlete will generate 20% and 35% of their body weight while testing the hip rotators and abductors, respectively (Fig. 2).
The hip rotator test is particularly accurate at predicting ACL injuries and is incredibly simple to perform. Of the 531 athletes tested, only 1% of the athletes who hit their target strength numbers tore their ACL, while 7% of athletes who did not tore the ACL in the following season.
Once identified, these athletes should be encouraged to participate in an ACL injury prevention program. These simple programs have been proven to decrease the rate of ACL tears by as much as 70%.5
Challenges With Traditional Return-to-Sport Protocols
It is also important to identify which athletes are prone to reinjury following surgical reconstruction, as ACL reinjury rates can be as high as 15%.6 To that end, various experts have developed return-to-sport protocols, which theoretically prevent reinjury by waiting until the athlete has full restoration of function before returning to the playing field.
One of the most widely used parameters for return to sport is to measure horizontal distance covered during various hop tests. When asymmetry is discovered, the athlete performs rehabilitative exercises until the distance covered is symmetric on both sides. Hop tests have been widely adopted by the rehab community, mostly because they are believed to duplicate on-field stresses associated with sport and do not require expensive equipment.
Regrettably, recent research has proven that these tests are poor indicators of knee joint function, as they unable to predict successful return to sport one year following injury.7 Additionally, upon returning to sport using these metrics, the athletes perform poorly8 and reinjury rates remain high.9 As a result, some experts suggest abandoning hop tests as a return-to-sport metric.10
Better Tests: The Single-Leg Jump and Single-Leg Drop
In 2022, researchers from Norway demonstrated that rather than evaluating hop distance, a more sensitive barometer for return to sport following ACL reconstruction is single-leg vertical jump performance.11 These tests are easy to administer, with the simplest being the single-leg jump test (SLJ).
To perform this test, have the athlete stand on one leg, drop to a self-selected depth, and then jump vertically with maximum effort and land on the same leg. Vertical height distance can be compared bilaterally.
An alternate way to perform this test is with the single-leg drop jump (SLDJ). The test is performed by having the athlete drop off of a 15-cm step and jump vertically, landing on the same leg.
The authors of this study show that previously injured athletes who had been cleared for return to sport using the hop distance protocols had significant impairments in single-leg jump performance. Specifically, even though athletes following ACL reconstruction achieved 97% symmetry in horizontal hop distance, only 83% and 77% were symmetric in the single-leg vertical jump and single-leg drop jump test, respectively.
Don't Overlook Soleus Weakness
Importantly, the authors also did an EMG analysis of every muscle in the hip, knee and leg as athletes performed the jump tests, and concluded that weakness of the soleus muscle was the single best predictor of poor performance. This research finding is extremely important, as most ACL prevention programs focus on improving neuromuscular deficits in the quads, glutes and hamstrings, while the soleus muscle is often completely overlooked.
This is troubling, as a growing body of research is showing that the soleus muscle plays a pivotal role in preventing anterior cruciate ligament injuries.12-13 In fact, research from Australia shows that because the soleus limits anterior translation of the tibia, it provides greater protection to the anterior cruciate ligament than all of the hamstrings combined.13
By pulling the tibia posteriorly during initial ground contact, the soleus keeps the knee aligned while the gluteus medius and the hip rotators prevent excessive internal femoral rotation. Preventing valgus collapse is one of the most important aspects of ACL rehab, but all too often clinicians overly focus on just the hip musculature.
Soleus Strengthening Exercises
My favorite way to strengthen the soleus is with bent-knee heel raises. To access all fibers of the soleus, I have the athlete move the rearfoot from full inversion to full eversion as they dorsiflex / plantarflex the ankle (Fig. 3).
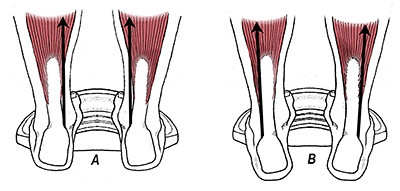 FIG 3 When performing bent-knee heel raises, it is important to move the rearfoot from full inversion to full eversion. Performing heel raises with the rearfoot everted targets the medial soleus (A), while inverting the rearfoot targets the lateral soleus (B). Plyometric drills incorporating various sideward and backward single-leg jumps are also effective for accessing all fibers of the soleus muscle.
When the athlete is ready, plyometric drills should be prescribed to improve agility, and an ACL prevention protocol should be initiated.5 Any restricted joints also should be manipulated – particularly the ankle joints, as manual therapies targeting the foot and ankle have been proven to increase hip strength and muscle activation,14 and enhance sensory motor control of the entire lower extremity.15
FIG 3 When performing bent-knee heel raises, it is important to move the rearfoot from full inversion to full eversion. Performing heel raises with the rearfoot everted targets the medial soleus (A), while inverting the rearfoot targets the lateral soleus (B). Plyometric drills incorporating various sideward and backward single-leg jumps are also effective for accessing all fibers of the soleus muscle.
When the athlete is ready, plyometric drills should be prescribed to improve agility, and an ACL prevention protocol should be initiated.5 Any restricted joints also should be manipulated – particularly the ankle joints, as manual therapies targeting the foot and ankle have been proven to increase hip strength and muscle activation,14 and enhance sensory motor control of the entire lower extremity.15
Clinical Takeaway
While no one would argue the importance of strengthening the glutes, quads and hamstrings when rehabilitating ACL injuries, the latest research is showing you get the best outcomes when you focus on improving function along the entire kinetic chain.
References
- Moses B, Orchard J, Orchard J. Systematic review: annual incidence of ACL injury and surgery in various populations. Res Sports Med, 2012;20(3-4):157-179.
- Feucht M, Cotic M, Saier T, et al. Patient expectations of primary and revision anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc, 2016;24:201-207.
- Ardern C, Taylor N, Feller J, et al. Fifty-five percent return to competitive sport following anterior cruciate ligament construction surgery: an updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br J Sports Med, 2014;48:1543-155.
- Khayambashi K, Ghoddosi N, Straub R, et al. Hip muscle strength predicts noncontact anterior cruciate ligament injury in male and female athletes: a prospective study. Am J Sports Med, 2015;(44):355-361.
- Gilchrist J, Mandelbaum H, et al. A randomized controlled trial to prevent noncontact anterior cruciate ligament injury in female collegiate soccer players. Am J Sports Med, 2008;36:1476-1483.
- Wiggins A, Grandhi R, Schneider D, et al. Risk of secondary injury in younger athletes after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Am J Sports Med, 2016;44:1861-1876.
- Ardern C, Webster K, Taylor N, et al. Return to the preinjury level of competitive sport after anterior cruciate ligament reconstruction surgery: two- thirds of patients have not returned by 12 months after surgery. Am J Sports Med, 2011;39:538-43.
- Niederer D, Engeroff T, Wilke J, et al. Return to play, performance, and career duration after anterior cruciate ligament rupture: a case- control study in the five biggest football nations in Europe. Scand J Med Sci Sports, 2018;28:2226-33.
- Wiggins A, Grandhi R, Schneider D, et al. Risk of secondary injury in younger athletes after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Am J Sports Med, 2016;44:1861-76.
- Kotsifaki A, Whiteley R, Van Rossom S, et al. Single leg hop for distance symmetry masks lower limb biomechanics: time to discuss hop distance as decision criterion for return to sport after ACL reconstruction? Br J Sports Med, 2022;56:249-56.
- Kotsifaki A, Van Rossom S, Whiteley R, et al. Single leg vertical jump performance identifies knee function deficits at return to sport after ACL reconstruction in male athletes. Br J Sport Med, 2022;56(9):490-498.
- Elias J, Faust A, Chu Y, et al. The soleus muscle acts as an agonist for the anterior cruciate ligament: an in vitro experimental study. Am J Sports Med, 2003; 31:241.
- Maniar N, Schache A, Pizzolato C, et al. muscle contributions to tibiofemoral shear forces and valgus rotational joint movements during single leg drop landing. Scand J Med Sci Sports, 2020 Sep;30(9):1664-1674.
- Lawrence M, Raymond J, Look E, et al. Effects of tibiofibular and ankle joint manipulation on hip strength and muscle activation. JMPT, 2020 Jun;43(5):406-417.
- McKeon P, Wikstrom E. Sensory-targeted ankle rehabilitation strategies for chronic ankle instability. Med Sci Sports Exerc, 2016;48:776-784.
Click here for more information about Thomas Michaud, DC.