






National and international treatment guidelines follow a common treatment path for patients with subacromial shoulder pain, also called shoulder impingement syndrome. As a first line of care, they recommend over-the-counter medications (e.g., NSAIDs, acetaminophen) and physical therapy elements (e.g., therapeutic rehabilitation, manual therapy).
Surgery: Common ... But Ineffective
Painful shoulders pose a substantial socioeconomic burden, accounting for 4.5 million physician visits annually in America.1 Subacromial pain accounts for up to 70 percent of all shoulder pain problems, and can impair the ability to work and do normal, everyday activities.
 Subacromial decompression was introduced in 1972 without high-level evidence as a treatment for subacromial shoulder pain. It is now one of the most common surgical procedures in orthopedics. More than 300,000 rotator-cuff repairs are performed annually in the United States, with annual direct medical costs estimated at more than $7 billion.2-3 However, the effectiveness of this procedure is uncertain. Let's examine the data from two clinical trials.
Subacromial decompression was introduced in 1972 without high-level evidence as a treatment for subacromial shoulder pain. It is now one of the most common surgical procedures in orthopedics. More than 300,000 rotator-cuff repairs are performed annually in the United States, with annual direct medical costs estimated at more than $7 billion.2-3 However, the effectiveness of this procedure is uncertain. Let's examine the data from two clinical trials.
The Research Doesn't Lie
Beard, et al., conducted a clinical trial to assess the effectiveness of surgical decompression in patients with subacromial shoulder pain.4 This study, published in Lancet, was a randomized, placebo-controlled, three-group trial. Participants were patients who had subacromial pain for at least three months, but without a full-thickness torn rotator cuff.
Participants were randomly assigned (1:1:1) to arthroscopic subacromial decompression (removing bone spurs and soft tissue), placebo decompression (skin incision and water irrigation), or no treatment.
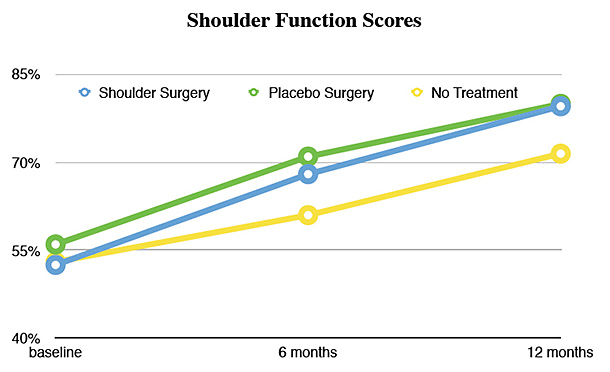
The graph titled "Shoulder Function Scores" demonstrates the results of the study. Function scores range from 0-100%, with a score of 100 percent indicating no shoulder symptoms or limitations in activities. Scores did not differ between the two surgical groups at six months or 12 months.
Both surgical groups showed a small benefit over no treatment, but real surgery was not better than placebo surgery. Conclusion: The surgical removal of bone spurs and soft tissue confers no benefit.
Paavola, et al., performed a randomized, double-blind, controlled trial to assess the efficacy of arthroscopic subacromial decompression by comparing it with diagnostic arthroscopy (a placebo surgical intervention).5 This study was published in the British Journal of Sports Medicine. Patients with a full-thickness torn rotator cuff were excluded.
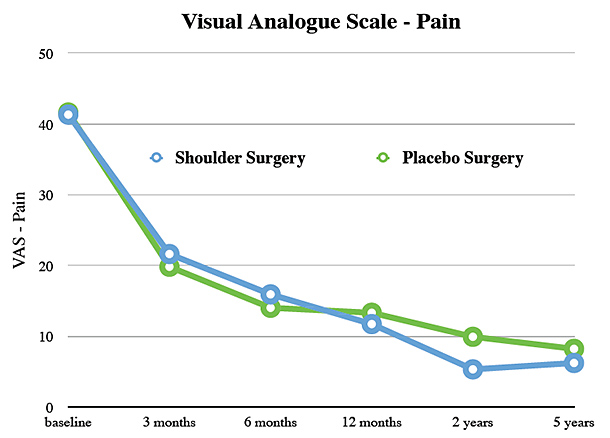
The graph titled "Visual Analogue Scale – Pain" demonstrates the results of this study. The visual analogue scale scores pain from 0 to 100, with 0 denoting no pain. Pain scores did not differ between the two surgical groups at any point in time over a five-year follow-up period. Conclusion: The surgical removal of bone spurs and soft tissue confers no benefit.
Surgery in both of these clinical studies failed. Moreover, the surgical complication rate for arthroscopic shoulder procedures is reported as 7.9 percent.6 Patients with subacromial shoulder pain lesions should consider a different strategy.
Steroid Injections: No Better
Steroid injections are also not effective in subacromial shoulder pain and can lead to serious adverse events including increased risk of osteoporosis, fracture and collagen necrosis.7-8
Chiropractic Care: The Superior Choice
Systematic reviews and randomized clinical trials support the following interventions for patients with subacromial pain: manual therapy, therapeutic rehabilitation, acupuncture and low-level laser therapy.9-11 These interventions can reduce pain, improve function and increase range of motion without serious adverse events. This strategy includes the primary therapies in our chiropractic package of care.
A New Paradigm
Health care professionals and insurance companies need to consider a new paradigm. A conservative package of care for subacromial shoulder pain is the most effective and safe option for patients, and surgery should not be considered as another option. Although a few patients (those with a full-thickness torn rotator cuff) may need surgery, most patients with subacromial shoulder pain do not.
References
- Oh LS, Wolf BR, Hall MP, et al. Indications for rotator cuff repair: a systematic review. Clin Orthop Relat Res, 2007;455:52-63.
- Jain NB, HigginsLD, Losina E, et al. Epidemiology of musculoskeletal upper extremity ambulatory surgery in the United States.BMC Musculoskelet Disord, 2014;15:4.
- Li L, Bokshan SL, Ready LV, Owens BD. The primary cost drivers of arthroscopic rotator cuff repair surgery: a cost-minimization analysis of 40,618 cases. J Shoulder Elbow Surg, 2019;28:1977-1982.
- Beard DJ, Rees JL, Cook JA, et al.; CSAW Study Group. Arthroscopic subacromial decompression for subacromial shoulder pain (CSAW): a multicentre, pragmatic, parallel group, placebo-controlled, three-group, randomised surgical trial. Lancet, 2018;391:329-338.
- Paavola M, Kanto K, Ranstam J, et al.; Finnish Shoulder Impingement Arthroscopy Controlled Trial (FIMPACT) investigators. Subacromial decompression versus diagnostic arthroscopy for shoulder impingement: a 5-year follow-up of a randomised, placebo surgery controlled clinical trial. Br J Sports Med, 2021;55:99-107.
- Shin JJ, Popchak AJ, Musahl V, Irrgang JJ, Lin A. Complications after arthroscopic shoulder surgery: a review of the American Board of Orthopaedic Surgery database. J Am Acad Orthop Surg Glob Res Rev, 2018;2:e093.
- Cook T, Minns Lowe C, et al. Are corticosteroid injections more beneficial than anaesthetic injections alone in the management of rotator cuff-related shoulder pain? A systematic review. Br J Sports Med, 2018;52:497-504.
- Dean BJ, Franklin SL, Murphy RJ, et al. Glucocorticoids induce specific ion-channel-mediated toxicity in human rotator cuff tendon: a mechanism underpinning the ultimately deleterious effect of steroid injection in tendinopathy? Br J Sports Med, 2014;48:1620-6.
- Hawk C, Minkalis AL, Khorsan R, et al. Systematic review of nondrug, nonsurgical treatment of shoulder conditions. J Manipulative Physiol Ther, 2017;40:293-319.
- Molsberger AF, Schneider T, Gotthardt H, Drabik A. German Randomized Acupuncture Trial for chronic Shoulder Pain (GRASP) - a pragmatic, controlled, patient-blinded, multi-centre trial in an outpatient care environment. Pain, 2010;151:146-154.
- Steuri R, Sattelmayer M, Elsig S, et al. Effectiveness of conservative interventions including exercise, manual therapy and medical management in adults with shoulder impingement: a systematic review and meta-analysis of RCTs. Br J Sports Med, 2017;51:1340-1347.
Click here for more information about Ronald Feise, DC.