






The criteria for the diagnosis of congenital dislocation of the hip include both physical and radiographic findings. Certain clinical signs have been identified that are helpful in the evaluation of newborns and infants for possible CHD, which include the following:
- limited abduction of the flexed hip, due to shortening and contraction of the hip adductors;
- increase in depth or asymmetry of the inguinal or thigh skinfolds;
- shortening of one leg;
- Allis' or Galeazzi's sign -- lower position of knee of the affected side when knees and hips are flexed, due to location of femoral head posterior to acetabulum in this position;
- Ortolani's "jerk" sign ("clunk of entry" or reduction sign);
- Barlow's test ("clunk of exit" or dislocation sign);
- telescoping or pistoning action of thighs, due to lack of containment of femoral head with acetabulum;
- Trendelenburg's test -- drop of normal hip when child, standing on both feet, elevates unaffected limb and bears weight on affected side, due to weakness of hip abductors; and
- waddling type of gait.
There are characteristic radiographic presentations which are present in each of the stages of CHD. The term congenital hip dysplasia generally refers to delayed or defective development of the hip joint leading to a deranged articular relationship between an abnormal acetabulum and a deformed proximal end of the femur. This condition is considered a precursor of the clinical entities of subluxation and dislocation of the hip.
In congenital subluxation of the hip, there is an abnormal relationship between the femoral head and acetabulum, but the two are in contact. Congenital dislocation of the hip, on the other hand, is associated with a complete loss of contact of the femoral head with the acetabular cartilage.
Unfortunately, the femoral head and acetabulum in the newborn cannot be assessed by direct visualization, since the femoral head is not ossified and is a cartilaginous body which is not visualized on plain films. The ossification center for the femoral head generally appears between three and six months; a delay in its appearance is an indication of congenital hip dysplasia. The neck of the femur is used for ascertaining the relationship between the acetabulum and the femoral head until the ossification center appears. The measurement used to evaluate the relationship of the femoral head and acetabulum include Hilgenreiner line, acetabular index, Perkin-Ombredanne line, Shenton-Menard line, and Andren-von Rosen line. (Figures 1 and 2)
The principal treatment for CHD is conservative, especially if diagnosed early. The most common technique is to reduce the dislocation of the femoral head by means of a flexion/abduction maneuver, for a sufficient period of time to permit proper growth of the head and acetabulum, which in turn assures a congruent and stable hip joint. This technique is usually performed on patients in the very early stages of CHD and in infants under two years of age; which include splinting, with a Frejka splint or Pavlik harness. Colonna or Buck's skin traction is used in children 2 to 12 years of age, with a well-padded spica cast applied simultaneously to the unaffected side.
If the conservative approach fails, or the child is too old, or the deformities are too advanced, surgical management is indicated. There are several surgical techniques currently in use for treating CHD, the most popular being the Salter osteotomy of the innominate bone, which may be combined with simultaneous derotation varus osteotomy of the femoral neck. The key to preventing significant deformities and future arthrosis of the hip is to diagnose CHD early, before the child begins to walk, when conservative care is most effective, and before the femoral head has completely ossified.
Reference: Information obtained from Orthopedic Radiology by Adam Greenspan, J.B. Lippincott 1988.
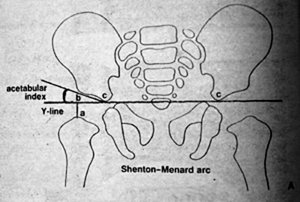
Figure 1 (A) Shenton-Menard Arc
The Hilgenreiner or Y-line is a line drawn through the superior part of the triradiate cartilage. In normal infants, the distance represented by a line (ab) perpendicular to the Y-line at the most proximal point of the femoral neck should be equal on both sides of the pelvis, as should the distance represented by a line (bc) drawn coincident with the Y-line medially to the acetabular floor. In infants age six to seven months, the mean value for the distance (ab) has been determined to be 19.3 mm +/- 1.5 mm; for the distance (bc), 18.2 mm +/- 1.4 mm. The acetabular index is an angle formed by a line drawn tangent to the acetabular roof from point (c) at the acetabular floor on the Y-line. The normal value of this angle ranges from 25 degrees to 29 degrees. The Shenton-Menard line is an arc running through the medial aspect of the femoral neck at the superior border of the obturator foramen. It should be smooth and unbroken.
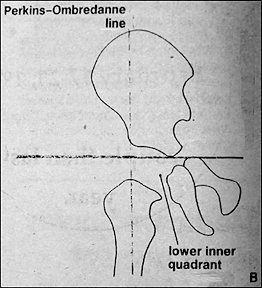
Figure 1 (B) Perkins-Ombredanne Line
The Perkins-Ombredanne line is drawn perpendicular to the Y-line, through the most lateral edge of the ossified acetabular cartilage, which actually corresponds to the anteroinferior iliac spine in normal newborns and infants, the medial aspect of the femoral neck or the ossified capital femoral epiphysis falls in the lower inner quadrant. The appearance of either of these structures in the lower outer or upper outer quadrant indicates subluxation or dislocation of the hip.
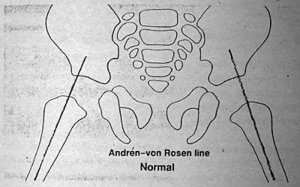
Figure 2 (A) The Andren-von Rosen Line -- Normal
The Andren-von Rosen line,, which is obtained with at least 45 degrees of hip abduction and internal rotation, is drawn along the longitudinal axis of the femoral shaft. In normal hips, it intersects the pelvis at the upper edge of the acetabulum.
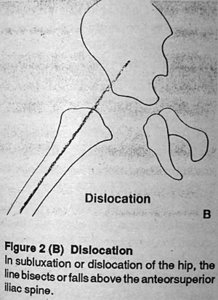
Figure 2 (B) Dislocation
In subluxation or dislocation of the hip, the line bisects or falls above the anteorsuperior iliac spine.
Deborah Pate, D.C., D.A.C.B.R.
San Diego, California
Editor's Note:
Dr. Pate's new book, Case Studies in Chiropractic Radiology is now available through MPI's Preferred Reading and Viewing List. Please see page xx for further information on how to order your copy.
Click here for more information about Deborah Pate, DC, DACBR.