





When the sciatic nerve is compressed or irritated by the piriformis muscle, causing pain, tingling and numbness in the buttocks and along the sciatic nerve, traveling through the posterior thigh and into the lower leg, it is called piriformis syndrome.
Presentation
The piriformis muscle originates from the anterior surface of the sacrum and inserts into the femur head. (Fig. 1) A herniated disc may result in compression / irritation of spinal nerve roots, creating sciatic-like nerve pain. Spinal nerve-root compression may be present, but not causal, in sciatica due to piriformis syndrome. Studies of spinal disc disease show a high frequency of abnormal discs in asymptomatic patients.1 The syndrome is most likely due to overuse or strain of the piriformis muscle.
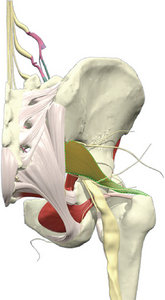 Fig. 1 The sciatic nerve runs under / through / over the piriformis muscle.
Complaints associated with the syndrome may include pain that is relieved by walking with the involved-side foot pointing outward. This position externally rotates the hip, reducing the stretch on the piriformis and sciatic nerve. Piriformis syndrome is also known as "wallet sciatica" or "fat wallet syndrome," as the condition can be caused or aggravated by sitting with a large wallet in the affected side's rear pocket.2 The external foot rotation should decrease as the muscle is corrected toward a normal tone.
Fig. 1 The sciatic nerve runs under / through / over the piriformis muscle.
Complaints associated with the syndrome may include pain that is relieved by walking with the involved-side foot pointing outward. This position externally rotates the hip, reducing the stretch on the piriformis and sciatic nerve. Piriformis syndrome is also known as "wallet sciatica" or "fat wallet syndrome," as the condition can be caused or aggravated by sitting with a large wallet in the affected side's rear pocket.2 The external foot rotation should decrease as the muscle is corrected toward a normal tone.
Diagnosis
Physical-exam findings include tenderness and weakness in the piriformis muscle. The pain is exacerbated with activity, prolonged sitting or walking.
The diagnosis is one of exclusion. Stretching the irritated piriformis and provoking sciatic nerve compression is performed by using the FABER (flexion, abduction, external rotation) and FAIR (flexion, adduction, internal rotation) maneuvers. Conditions to be ruled out include disc herniation, facet arthropathy, spinal stenosis and lumbar muscle strain.3
 Fig. 2 Strength testing the piriformis.
Look for a loss of range motion and/or a loss of coordination with the FAIR motion. Muscle test bilaterally and note the deficiency of the involved piriformis. Muscle testing involves having the patient lie prone with knee flexed and lower leg internally rotated. Grasp the patient's elevated ankle and pull the lower leg toward midline. (Fig. 2)
Fig. 2 Strength testing the piriformis.
Look for a loss of range motion and/or a loss of coordination with the FAIR motion. Muscle test bilaterally and note the deficiency of the involved piriformis. Muscle testing involves having the patient lie prone with knee flexed and lower leg internally rotated. Grasp the patient's elevated ankle and pull the lower leg toward midline. (Fig. 2)
Treatment
In one study, a "sciatic nerve press," in which pressure was applied simultaneously to the sciatic nerves at the back of both thighs, resulted in immediate relief of pain. Peak pain relief occurred after between 10 and 20 minutes, and the relief decreased by 47 percent by the 60th minute, according to the study.4
 Fig. 3 Piriformis correction. Press into the origin and hold 3-5 seconds.
Effectively correcting the piriformis dysfunction involves reducing the hypertonic state. Thrusting and/or pressing into the sciatic notch will affect the fibers at the origin, while forces applied at the femur head will address the insertion fibers. Press and hold for 3-5 seconds into these areas in order to stimulate the golgi tendon organs and reduce hypertonicity. (Fig. 3) Post-treatment evaluation should note increased strength and FAIR range of motion, along with reduced pain.
Fig. 3 Piriformis correction. Press into the origin and hold 3-5 seconds.
Effectively correcting the piriformis dysfunction involves reducing the hypertonic state. Thrusting and/or pressing into the sciatic notch will affect the fibers at the origin, while forces applied at the femur head will address the insertion fibers. Press and hold for 3-5 seconds into these areas in order to stimulate the golgi tendon organs and reduce hypertonicity. (Fig. 3) Post-treatment evaluation should note increased strength and FAIR range of motion, along with reduced pain.
Rehabilitation
Stretch the piriformis with the patient lying supine by bringing the involved-side bent leg across the body and up toward the opposite shoulder. While maintaining this stretch, the tender piriformis fibers can be massaged to release more muscle fiber tension.
Strengthening the piriformis can be achieved by performing side-lying clam exercises and quadruped hip abduction. I prefer my patients work the good side first and then train the involved side.
Quadruped Hip Abduction: Beginning position is an all-fours position. Instruct patient to keep their knee bent and lift the involved leg in the air to the side until it parallels the floor. This can be done using multiple sets and reps without resistance; or exercise tubing can be used to add resistance.
Side-Lying Clam Exercise: Instruct patient to lie on their side with the involved hip on top; then bend their knees, keep the ankles together and raise the top knee away from the bottom one. Again, this can be done using multiple sets and reps without resistance, or exercise tubing can be used to add resistance.
References
- Deyo RA, Weinstein JN. Low back pain. New Engl J Med, 2011 Feb;344(5):363-70.
- Piriformis Syndrome (Hip/Buttocks Pain).
- Kirschner JS, Foye PM, Cole JL. Piriformis syndrome, diagnosis and treatment. Muscle & Nerve, 2009 Jul;40(1):10-18.
- Jiman He, et al. A new analgesic method, two-minute sciatic nerve press, for immediate pain relief: a randomized trial. BMC Anesthesiol, 2008;8:1.
Dr. Todd Turnbull, has authored online courses and articles about concussions, sports performance, soft-tissue diagnosis, rehabilitation and disc herniations. He is a 1991 graduate of Life University, a board-certified chiropractic sports physician, and maintains a private practice in Portland, Ore. He can be contacted with questions or comments via his Web site: www.drtoddturnbull.com/DCJournal.