





The prevalence of neck pain is significant in the general population, affecting 30-50 percent in a 12-month period, with a lifetime prevalence exceeding 70 percent.1-2 With that said, let's focus on the effects of chiropractic spinal adjustments (CSA) on cervical spine outcomes regarding pain and biomechanical functional outcomes.
The original reporting of joint gapping by Cramer, et al. (2002),3 and more recent reporting by Anderst, et al. (2018),4 utilized a chiropractic spinal adjustment performed by an experienced chiropractor. Therefore, we focus on chiropractic to prevent confusion when considering a care path based on an evidence-based model.
Cramer, et al., reported that "the thrust given during the chiropractic procedure had the effect of increasing the gapping of the Z joints. The average difference between the control subjects…and the subjects that received a chiropractic adjustment and remained in the side-posture position was 1.33 mm ... a difference of 0.71 mm was found between the side-posture group." Anderst, et al., reported, "The facet gap increased 0.9 +/- 0.40.")
The evidence 16 years apart is consistent, with the most current article validating biomechanical changes as a direct result of a chiropractic spinal adjustment. Anderst, et al., also reported, "The results suggest that clinical and functional improvement after manipulation (CSA) may occur as a result of small increases in intervertebral ROM across multiple motion segments. This study demonstrates the feasibility of characterizing in real-time the manual inputs and biological responses that comprise cervical manipulation (CSA), including clinician-applied force, facet gapping, and increased intervertebral ROM."
Beyond post-MRI, which is unrealistic in clinical practice due to the cost, there are algorithms based on X-ray to help diagnose biomechanical changes and normalization of the spine. Muth-Seng, et al. (2022),5 reported, "The study of the subsequent subject-specific spinal loading could help further the understanding of cervical spine biomechanics, degeneration mechanisms, and complications. We also know, despite the political rhetoric, that diagnostic x-ray is safe and has no carcinogenic effect."
Tubiana, et al. (2009),6 reported, "Among humans, there is no evidence of a carcinogenic effect for acute irradiation". Diagnostic x-rays have had virtually no negative adverse health sequelae based upon this and the totality of other literature."
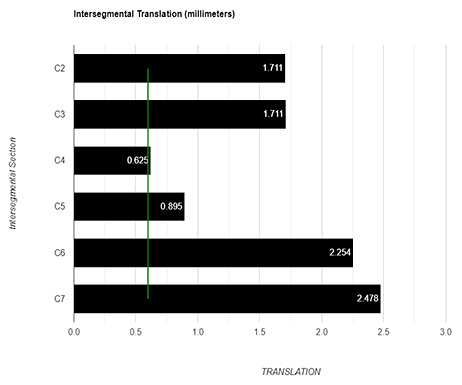
There are digitizing tools that render pre- and-post spinal biomechanics based on X-ray and ligamentous physiology to demonstratively document changes. They also render visual evidence of permanent changes. Note the green line on the graph, indicating the ligament's para physiological pathological limit.7
This is a clinical demonstrative indicator, based upon X-ray and devoid of side effects, to show the facets reintegrating (or lack thereof) post-CSA based upon normalizing spinal biomechanics.
Take-Home Points
Anderst, et al., concluded: "The results demonstrate that target and adjacent motion segments undergo facet joint gapping during manipulation and that intervertebral ROM is increased in all three planes of motion after manipulation. The results suggest that clinical and functional improvement after manipulation (CSA) may occur as a result of small increases in intervertebral ROM across multiple motion segments. This study demonstrates the feasibility of characterizing in real-time the manual inputs and biological responses that comprise cervical manipulation, including clinician-applied force, facet gapping, and increased intervertebral ROM."
Studies implicate the cervical facet joint and its capsule as a primary anatomical site of injury during whiplash exposures to the neck. Biomechanical investigations of the neck during whiplash simulations indicate that the cervical spine exhibits an abnormal S-shaped curve in which the primary motions of the vertebrae in the lower cervical spine is posterior retraction relative to their inferior adjacent vertebrae.8
Hauser, et al., reported that once ligaments have been compromised, they never heal. They would repair with collagen replacing collagen and elastin, leaving "Strain/Sprain injury permanent no matter how minimal the tissue damage.9 Contemporary analytical digitizing tools can assess the locations of facet compromise for accurate treatment planning of the primary spinal lesion and the necessity for care.
DISCLOSURE: The authors declare that they have a financial interest that relate to the findings described in this paper.
References
- Hogg-Johnson S, van der Velde G, Carroll LJ, et al. The burden and determinants of neck pain in the general population: results of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. Spine, 2008;33(4 Supp l):S39-51.
- Fejer R, Kyvik KO, Hartvigsen J. The prevalence of neck pain in the world population: a systematic critical review of the literature. Eur Spine J, 2006;15:834-48.
- Cramer GD, Gregerson DM, Knudsen, JT, et al. The effects of side-posture positioning and spinal adjusting on the lumbar Z joints: a randomized controlled trial with sixty-four subjects. Spine, 2002;27(22):2459-2466.
- Anderst W, et al. "Intervertebral kinematics of the cervical spine before, during, and after high-velocity low-amplitude manipulation. Spine J, 2018;18(12):2333-2342.
- Muth-Seng C, et al. Personalized gravitational loading of the cervical spine from biplanar X-rays for asymptomatic and clinical subjects in neutral standing position. Clin Biomech, 2022:105577.
- Tubiana M, Feinendegen LE, Yang C, Kaminski JM. The linear no-threshold relationship is inconsistent with radiation biologic and experimental data. Radiology, 2009;251(1):13-22.
- Lin RM, Tsai KH, Chu LP, Chang PQ. Characteristics of sagittal vertebral alignment in flexion determined by dynamic radiographs of the cervical spine. Spine, 2001;26(3):256-261.
- Lee DJ, Winkelstein, BA. The failure response of the human cervical facet capsular ligament during facet joint retraction. J Biomech, 2012;45(14):2325-2329.
- Hauser RA, Dolan EE, Phillips HJ, et al. Ligament injury and healing: a review of current clinical diagnostics and therapeutics. Open Rehabil J, 2013;6(1).
Dr. Mark Studin is an adjunct associate professor at the University of Bridgeport School for Chiropractic, teaching advanced imaging and triaging chronic and acute patients; and an adjunct postdoctoral professor at Cleveland University-Kansas City College of Chiropractic. He is also a clinical instructor for the State University of New York at Buffalo, Jacobs School of Medicine and Biomedical Sciences, Office of Continuing Medical Education. Dr. Studin consults for doctors of chiropractic, medical primary care providers and specialists, and teaching hospitals nationally. He can be reached at
![]() or 631-786-4253.
or 631-786-4253.
Dr. Don Capoferri has been practicing in the Atlanta, Ga., area since 1982. After completing his undergraduate education at Rutgers University, he earned his DC degree at Pennsylvania College of Chiropractic, graduating in December of 1981. After a two-year course of study, internship and research, he was the first chiropractor in the nation to receive a fellowship in spinal biomechanics and trauma from Cleveland University, Chiropractic and Health Sciences (where he is currently an adjunct professor of clinical sciences). Dr. Capoferri has extensive postgraduate training and credentials in MRI spine interpretation, spinal biomechanical engineering, spinal trauma pathology and electrodiagnostics.