






The etiology of perineural sacral cysts (Tarlov's cysts) is not well-understood. The best description is that they are a dilatation of arachnoid and dura of spinal posterior nerve-root sheath, containing nerve fibers.
 These cysts can occur anywhere in the spine, but the most common areas affected are the S-2 and S-3 nerve roots. Sacral cysts have been reported to cause sacral radiculopathy, hip, leg or foot pain, perineal pain, paresthesias, and bowel or bladder dysfunction. Symptoms can mimic a disc herniation.
These cysts can occur anywhere in the spine, but the most common areas affected are the S-2 and S-3 nerve roots. Sacral cysts have been reported to cause sacral radiculopathy, hip, leg or foot pain, perineal pain, paresthesias, and bowel or bladder dysfunction. Symptoms can mimic a disc herniation.
There are many variations of Tarlov cysts. Some can become quite large - up to 6 cm. They can be multiple. As you might suspect, there is some confusion over the precise definition of Tarlov cysts and how they are different from other spinal cysts. The distinctive feature of the Tarlov perineurial cyst is the presence of spinal nerve root fibers within the cyst wall or cyst cavity itself.
The nomenclature becomes daunting because the etiology of this lesion is still not agreed upon and unfortunately, there is no consensus on the optimal management of symptomatic Tarlov cysts. The good news is that most remain asymptomatic.
Treatment recommendations for symptomatic Tarlov cysts vary widely depending on the symptoms. They can be drained of CSF; in fact, draining the CSF also can be a useful diagnostic tool to determine if symptoms are indeed due to the Tarlov cyst. There are two ways of draining these cysts: one is via a lumboperitoneal shunt; the other is percutaneous drainage. Unfortunately, the cysts re-form over time with percutaneous aspiration.
Surgical treatment involves complete cyst removal and excision of the affected posterior root and ganglion. As you can imagine, there are several ways of doing this complete excision, which I will not describe here.
When I chose this topic to report upon, I didn't realize that there is an evolving specialty for treating these cysts. The classification and treatment procedures are evolving; therefore, I refer you to www.tarlovcyst.net for updated information.3
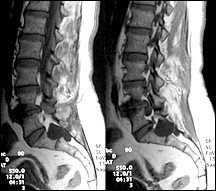
Unfortunately, there is no consensus yet as to the best way to manage these lesions. With improved imaging, these cystic lesions are becoming more apparent and most of the time they are considered incidental findings; the problem occurs when differentiating these cysts from other causes for the patient's symptoms, such as degenerative disc and joint disease.
It is interesting to note that even though the Tarlov cyst was described more than 60 years ago, we still have no agreement on the origin. They may be caused by inflammation, trauma or congenital weakness of the dura mater, combined with elevated CSF hydrostatic pressure. Regardless of the origin of the Tarlov cyst, treatment procedures are improving and most cases fortunately do not require any intervention.
References
- Paulsen RD, Call GA, Murtagh FR. Prevalence and percutaneous drainage of cysts of the sacral nerve root sheath (Tarlov cysts). AJNR 1994;15:293,297.
- Mummanei PV, Petts LH, McCormack BM, et al: Microsurgical treatment of symptomatic sacral Tarlov cysts. Neurosurgery 2000;47:74,79.
- Acosta F, Quinones-Hinojosa A, Schmidt M, Weinstein P. Diagnosis and management of sacral Tarlov cysts. Case report and review of the literature. Neurosurgy Focus 2003;15(2). www.aans.org/education/journal/neurosurgical/aug03/15-2-15.pdf.
Click here for more information about Deborah Pate, DC, DACBR.