






This article was inspired by a recent article by Robert Cooperstein, MA, DC.1 I find that I often end up being the physician of last resort, seeing patients who have not responded to previous chiropractic care, PT or medical management.
This leads directly to the cultural authority issue. Our profession is in a battle for its survival, with our territory being nibbled away by physical therapists and MDs. I don't think we can win this war by strictly being the best at spinal manipulation or by limiting the license of other providers. I believe we have to become the best at nonsurgical, nonpharmaceutical management of spinal pain syndromes. This means we have to be the very best physicians of the spine, using the lost arts of the history and physical exam, as well as modern imaging, to accurately and completely diagnose. It is about looking at the whole patient. And we have to teach our patients how to take care of themselves.
Most Missed Soft Tissue
Don't limit yourself to just breaking up tight muscular fascia. Think about what soft tissues are not helping stabilize the affected area. We can affect ligaments and make them more functional. Many of us do some kind of soft-tissue work to the gluteal origins from the iliac crest. In doing so, I think we are also affecting the long dorsal ligaments of the SI joint. What we often seem to miss are two key ligamentous structures. I wrote a whole article on this concept back in 2005.2
I didn't fully understand the iliolumbar ligament four years ago, so here is an addendum to that article. You can't just pay lip service to the iliolumbar; you have to find it and get deep to correct it. Your best bet for this is some kind of instrument-assisted soft-tissue technique. I prefer Graston Technique. You want to get to both the origin and the insertion of this ligament. The origin seems obvious, but is easily missed. It comes off of the iliac crest, but the origin is on the anterior side of the iliac crest. You cannot have the patient stretched out (such as bent forward, sitting in flexion), as your touch will be too superficial.
You need to slightly slack or relax the area. You can do this by having the sitting patient bend to the involved side and support themselves on their arm. Using your curled fingers, start over the L5 mammillary process, and slide laterally. Press anterolateral and slightly inferior from L5 to put tension on the ligament. You have to stay medial and roll forward with a superior to inferior pressure, toward the anterior surface of the iliac crest. You will find a tender spot or band. Now get out your Graston tools, or something similar, and do deep massage and deep friction work to these tissues. You can do this with your hands, but it is harder to be effective, takes more time and will wear out your hands.
The other end of this ligament is another spot that is routinely missed. The iliolumbar ligament inserts into transverse processes of L5 (and L4, in some cases). Again, if you push from posterior to anterior, you'll probably miss it, especially on patients who have some bulk. So, you have to start laterally above the iliac crest and push lateral to medial until you feel the insertion of the ligament into the bony prominence of the transverse process. If it's tender, it needs deep soft-tissue work.
Remember, ligaments are not supposed to be tender. If they are tender to the touch, they are likely contributing to the pain pattern in the lower back. The iliolumbar ligament is a key stabilizer for both the lower lumbar spine and for the sacroiliac joint The second critical soft-tissue area for the lower back is the sacrotuberous ligament. This was well-addressed in the 2005 article, so I won't repeat myself.
Most Missed Rehab
In the rehab of the lower back, I think that slow, low-load training of the deeper stabilizers is what is missed too often. I spent most of 2008 writing on this topic, so I reference my articles here in case you are interested in exploring this further.3-5
Most Missed Joint Dysfunctions
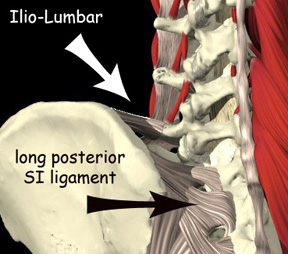 The iliolumbar ligament, seen from behind; note how the origin is hidden in the front of the iliac crest (courtesy of Primal Pictures).
I wouldn't be a technique writer without emphasizing the importance of manipulation to restricted joints. Most of us do a decent job on the iliosacral side of the articulation, but I suspect that many of us miss sacral restrictions or just pound down the high side of the sacral base. I have found that Mitchell's muscle-energy model really seems to stand the test of time for the assessment and correction of sacral problems. (I dislike the name of this technique. I would prefer to call it post-isometric relaxation for the joints.)
The iliolumbar ligament, seen from behind; note how the origin is hidden in the front of the iliac crest (courtesy of Primal Pictures).
I wouldn't be a technique writer without emphasizing the importance of manipulation to restricted joints. Most of us do a decent job on the iliosacral side of the articulation, but I suspect that many of us miss sacral restrictions or just pound down the high side of the sacral base. I have found that Mitchell's muscle-energy model really seems to stand the test of time for the assessment and correction of sacral problems. (I dislike the name of this technique. I would prefer to call it post-isometric relaxation for the joints.)
Despite its archaic terminology and the difficultly of grasping concepts framed differently than our usual chiropractic model, I find it very useful. I have used many models over the years, but I keep coming back to the classic muscle-energy model for looking at sacral restrictions. I haven't written about this in depth, but it is out there, used primarily by osteopaths and physical therapists.
Most of my chiropractic motion palpation is kinesthetic. I am feeling for an abnormal motion when I move a joint. The Gillet test uses a visual model, asking the patient to actively move the joint and watching for what doesn't move. If we go back to our basic Gillet stork test, we can assess both the iliac, non-weight-bearing side, and the sacral, weight-bearing side. I've demonstrated this on YouTube.6
 As the patient fully lifts the bent right leg, the right ilium rotates posterior, relative to the sacrum.
The patient stands in front of you, facing away. They can support themselves by having a hand on a chair or table; it is not primarily a balance test. For the right side of the SI, your contact is on the right PSIS with your right thumb, and just medial to the PSIS, on the right sacral base at the S1 or S2 level, with the left thumb. Your thumbs are parallel to each other, in the horizontal plane.
As the patient fully lifts the bent right leg, the right ilium rotates posterior, relative to the sacrum.
The patient stands in front of you, facing away. They can support themselves by having a hand on a chair or table; it is not primarily a balance test. For the right side of the SI, your contact is on the right PSIS with your right thumb, and just medial to the PSIS, on the right sacral base at the S1 or S2 level, with the left thumb. Your thumbs are parallel to each other, in the horizontal plane.
First, have the patient lift the right leg, bent at the knee, as high as they can. Does the ilium (PSIS) move inferiorly relative to the sacrum? If so, that is normal motion. If the ilium either stays level or goes anterior-superior, the iliosacral side of the joint lacks motion. Don't make it complex, just look for a basic motion. The ilium moving inferior as it saggitally rotates.
Next, test the weight-bearing mechanisms on the right side. Have the patient lift the left leg, bent at the knee, as high as they can. You are testing the right-side sacrum. Does it come back at you or appear to move inferior in relation to the PSIS? If so, this is normal motion. If not, there is a lack of motion of the sacral side of the joint.
 As the patient fully lifts the bent left leg, the sacrum moves inferior, relative to the right ilium.
Do this for all four joints of the SI. Don't get distracted by which side hurts. You want to know exactly where they are lacking motion. For the joints that don't move, do your usual manipulation or mobilization for correcting this. Go back to the Gillet test at the end and see if you have corrected the lack of motion. If not, you need to try some other form of manipulation for that joint. I've noticed that my previous motion-palpation assessments did not seem to always be accurate. The Gillet test, interpreted in this manner, seems to give me a better picture. I then use the muscle-energy model to assess and correct the sacral side of the dysfunction. (The muscle-energy model is a bit complex, so I will wait until I have a whole article to present it in detail.)
As the patient fully lifts the bent left leg, the sacrum moves inferior, relative to the right ilium.
Do this for all four joints of the SI. Don't get distracted by which side hurts. You want to know exactly where they are lacking motion. For the joints that don't move, do your usual manipulation or mobilization for correcting this. Go back to the Gillet test at the end and see if you have corrected the lack of motion. If not, you need to try some other form of manipulation for that joint. I've noticed that my previous motion-palpation assessments did not seem to always be accurate. The Gillet test, interpreted in this manner, seems to give me a better picture. I then use the muscle-energy model to assess and correct the sacral side of the dysfunction. (The muscle-energy model is a bit complex, so I will wait until I have a whole article to present it in detail.)
The other major lower back restriction that is frequently missed is in the midline of the lower lumbars. We seem to find the rotations, but often miss the midline. When the patient has midline tenderness and a lack of superior movement of a spinous process, I consider it a compression pattern. Test via a deep posterior to anterior, with simultaneous inferior to superior pressure. You are in the interspinous space, pushing superior on the inferior aspect of the spinous above.
I used to think this meant the disc was under tension, but there is not a whole lot of evidence to support that view. Maybe this reflects dural tension, a disc, the interspinous or supraspinous ligament, or just a smushed or compressed joint, either the facet or the disc space.7 Whatever the lesion really is, the midline problem needs to be corrected. Localized decompression is usually what corrects this, although sometimes the finding will disappear once I correct an SI or lumbar motion deficit. Use your flexion-distraction table, your vertebral distraction pump or your fancy decompression table. Show the patient how to decompress themselves and tell them to do this several times a day until the area is no longer tender.8
As usual, I've just scratched the surface. I hope these ideas improve your exam and treatment of difficult lower back patients. Even after 30 years of practice, I am still fascinated by the lower back and its problems.
References
- Cooperstein R. "Ten of My Favorite Clinical Chiropractic Trade Secrets, Part 1." Dynamic Chiropractic, Oct. 7, 2009.
- Heller M. "Sacro-Iliac Revisited, the Importance of Ligamentous Integrity." Dynamic Chiropractic, July 2, 2005.
- Heller M. "Core Stability Principles." Dynamic Chiropractic, Sept. 9, 2008. .
- Heller M. "Global Stabilizers for the Low Back." Dynamic Chiropractic, Oct. 21, 2008.
- Heller M. "Local Stabilizer Rehabilitation, Myths and Understandings." Dynamic Chiropractic, Dec. 2, 2908.
- Heller M. The Gillet (Stork) Test. www.youtube.com/user/marchellerdc#p/u
- Heller M. "Discogenic Pain, Diagnosis and Treatment." Dynamic Chiropractic, Sept. 1, 2003.
- Heller M. "Decompression, Myths and Models." Dynamic Chiropractic, Jan. 1, 2007.
Click here for more information about Marc Heller, DC.