






A motion deficit in all joints should be considered pathological. It appears, however, that loss of internal rotation in the shoulder and hip is related to more pathology than most other joints.
 Athletes who emphasize extreme, repetitive, external rotation of the glenohumeral joint will increase this range of motion and also will experience a decrease of internal rotation. It is thought that as long as the total arc of motion (internal and external) of the dominant arm equals the range of the nondominant arm, there will be relatively normal function.1 However, this is not necessarily true. Loss of internal rotation is not mandatory when gaining external rotation.2 Acquired loss of internal rotation (glenohumeral internal rotation deficit, or GIRD) is mostly considered a soft-tissue problem. Increased shoulder external rotation is more a bony adaptation, due to retroversion of the humerus. Increased external rotation at the glenohumeral joint allows greater velocity to be generated, and the retroverted position may help to stabilize the anterior force on the anterior capsule and ligaments1 during the cocking and acceleration phase of the throw.
Athletes who emphasize extreme, repetitive, external rotation of the glenohumeral joint will increase this range of motion and also will experience a decrease of internal rotation. It is thought that as long as the total arc of motion (internal and external) of the dominant arm equals the range of the nondominant arm, there will be relatively normal function.1 However, this is not necessarily true. Loss of internal rotation is not mandatory when gaining external rotation.2 Acquired loss of internal rotation (glenohumeral internal rotation deficit, or GIRD) is mostly considered a soft-tissue problem. Increased shoulder external rotation is more a bony adaptation, due to retroversion of the humerus. Increased external rotation at the glenohumeral joint allows greater velocity to be generated, and the retroverted position may help to stabilize the anterior force on the anterior capsule and ligaments1 during the cocking and acceleration phase of the throw.
 Of course, even with the retroversion and adaptive remodeling of the tissues, symptoms or injury may occur if the forces or stresses about the glenohumeral joint exceed the range of load acceptance.1 Symptoms in the skeletally immature patient may be due to physeal injury. In the skeletally mature patient, symptoms and injuries are often due to boney stress reactions, anterior capsulolabral laxity and eventual instability. Osbahr, et al., in evaluating the throwing shoulder of college baseball players, speculated that complaints of pain from the proximal physis of the humerus may have stemmed from when the athletes were skeletally immature, before their college baseball pitching careers began.1 Their pain could therefore be osseous in origin, while tendinous pain might not have subsided. Humeral osseous retroversion may be demonstrated by a single radiograph.1,3
Of course, even with the retroversion and adaptive remodeling of the tissues, symptoms or injury may occur if the forces or stresses about the glenohumeral joint exceed the range of load acceptance.1 Symptoms in the skeletally immature patient may be due to physeal injury. In the skeletally mature patient, symptoms and injuries are often due to boney stress reactions, anterior capsulolabral laxity and eventual instability. Osbahr, et al., in evaluating the throwing shoulder of college baseball players, speculated that complaints of pain from the proximal physis of the humerus may have stemmed from when the athletes were skeletally immature, before their college baseball pitching careers began.1 Their pain could therefore be osseous in origin, while tendinous pain might not have subsided. Humeral osseous retroversion may be demonstrated by a single radiograph.1,3
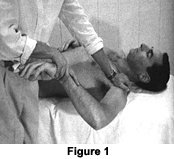
An important cause of GIRD is posterior capsule tightness. When the posterior capsule is tight, during external rotation, the humeral head translates more anteriorly than normal and is associated with the development of shoulder instability. With a tight posterior capsule during shoulder external rotation, there also can be stress to the posterior rotator cuff as the humeral head translates anteriorly. A significant limitation of internal rotation and posterior capsule tightness has been found to be associated with instability and impingement. Stretching of the posterior capsule and treatment of the posterior capsule using ART and Graston technique has clinically proven to solve this problem. Figure 1 depicts how to examine for range of internal rotation on a supine patient, with the examiner stabilizing the shoulder and scapula in 90 degree abduction while pushing down on the distal forearm. There should be at least 70 degrees of internal rotation.
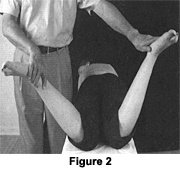
Hip evaluation of range of motion demonstrating a loss of internal rotation is always significant. Figure 2 depicts a prone patient with comparison of internal rotation for the hip. The right hip is limited. Limited, painful, internal hip rotation is found in internal derangements: slipped capital femoral epiphysis; muscular contracture (shortness of external hip rotators); sprain or partial rupture of the ischiofemoral ligament or the descending medial part of the iliofemoral ligament; hip bursitis (trochanteric, iliopectineal); or upper rectus tendonitis.4
Almost every hip osteoarthritis is associated primarily with decreased internal hip rotation, followed by reduced hip flexion.5 Loss of hip medial rotation with a hard end-feel is the first sign of osteoarthritis, followed by loss of hip flexion. As we age, the hip capsule becomes fibrotic and, because of the spiral arrangement of its fibers, taut, especially in medial rotation.
This pattern of limited passive motion is due to the capsular pattern of the hip, as described by Dr. Cyriax. The capsular pattern for most of the joints of the body that demonstrate a tight capsule (arthritis, arthrosis) or inflamed synovial tissue was established by Dr. Cyriax. The literature has agreed with most of his ideas regarding this concept over the past 50 to 60 years.4
References
- Osbahr DC, Dannon DL, Speer KP. Retroversion of the humerus in the throwing shoulder of college baseball pitchers. Am J Sports Med, 2002;30(3):347-353.
- Lintner D, Mayol M, Uzodinma O, et al. Glenohumeral internal rotation deficits in professional pitchers enrolled in an internal rotation stretching program. Am J Sports Med, 2007;35(4):617-21.
- Soderlund V, Kronberg M, Brostrom LA. Radiologic assessment of humeral head retroversion. Description of a new method. Acta Radiol, 1989;30(5):501-5.
- Hammer W. Functional Soft Tissue Examination & Treatment by Manual Methods, 3rd ed. Sudbury, Mass.: Jones & Bartlett, 2007.
- Altman R, Alarcon G, Appelrouth D, et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheum, 1991;34(5):505-14.
Click here for previous articles by Warren Hammer, MS, DC, DABCO.