





"Optimum spinal function requires proper balance of various anatomical structures. In chiropractic, radiographic analysis is a tool that aids in optimum patient care and trends have shifted from performing x-rays on almost everyone to radiographing almost no one - this approach is 'out of balance'."
-Terry R.
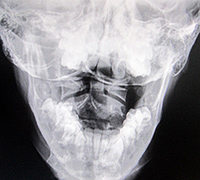 Fig. 1: A-P Open Mouth
The most important test to be performed on the structural fingerprint exam is the imaging, primarily the standing x-ray. Standing x-rays set us apart from every other profession who treat high school athletic injuries. No other profession takes or can read the biomechanical information found on standing x-rays, and these findings provide critically telling information, much of it being the predictability as to what areas of the musculoskeletal system are going to break down over time. Abnormal loading, regardless of symptomatology, will dictate the age at which this young athlete will no longer be able to participate in a given activity. Our goal is to detect these abnormal loadings, educate the patient as to their presence, and provide a custom, corrective program that will help this young athlete reach their maximum biomechanical potential. We need to be concerned with long term musculoskeletal wellness.
Fig. 1: A-P Open Mouth
The most important test to be performed on the structural fingerprint exam is the imaging, primarily the standing x-ray. Standing x-rays set us apart from every other profession who treat high school athletic injuries. No other profession takes or can read the biomechanical information found on standing x-rays, and these findings provide critically telling information, much of it being the predictability as to what areas of the musculoskeletal system are going to break down over time. Abnormal loading, regardless of symptomatology, will dictate the age at which this young athlete will no longer be able to participate in a given activity. Our goal is to detect these abnormal loadings, educate the patient as to their presence, and provide a custom, corrective program that will help this young athlete reach their maximum biomechanical potential. We need to be concerned with long term musculoskeletal wellness.
 Fig. 2: Digital Foot Scan
Law of Tissue Tolerance
Fig. 2: Digital Foot Scan
Law of Tissue Tolerance
When the loading of a tissue exceeds the capacity of that tissue, compensatory physiological changes occur. Such changes include joint fixation, spurs, inflammation, swelling, muscle restriction, degeneration, bone adaptation, fractures (avulsion, stress, hairline, etc.) and disc injury. In an effort to minimize exposure, we've developed a four view series that provides significant, detailed information about each athlete. The four views are: the A-P open mouth/lower cervical, the lateral cervical, the A-P lumbar and the lateral lumbar. It is appropriate for additional views to be taken if the examiner determines their need. All x-rays should be taken with shoes off.
 Fig. 3: Lateral Cervical (Normal)
In Figure 1, we can see significant imbalances. Many of these imbalances originate from the imbalances found in the feet and can be seen on the digital foot scan (Figure 2). Remember, the body is a compensatory mechanism and any disturbance between atlas, axis and the occiput are typically a compensation for the imbalances below. Therefore, for maximum biomechanical potential, you must address the feet imbalances first.
Fig. 3: Lateral Cervical (Normal)
In Figure 1, we can see significant imbalances. Many of these imbalances originate from the imbalances found in the feet and can be seen on the digital foot scan (Figure 2). Remember, the body is a compensatory mechanism and any disturbance between atlas, axis and the occiput are typically a compensation for the imbalances below. Therefore, for maximum biomechanical potential, you must address the feet imbalances first.
 Fig. 4: Lateral Cervical (Abnormal)
In Figure 1, we can see there is rotation of the axis, however, the right pillar of the atlas is wider than the left pillar of the atlas because the atlas, too, is rotated and the right pillar is closer to the tube. Finally, if you notice the open mouth, it too, is angled to the left, showing abnormal rotation in the occiput, atlas and axis.
Fig. 4: Lateral Cervical (Abnormal)
In Figure 1, we can see there is rotation of the axis, however, the right pillar of the atlas is wider than the left pillar of the atlas because the atlas, too, is rotated and the right pillar is closer to the tube. Finally, if you notice the open mouth, it too, is angled to the left, showing abnormal rotation in the occiput, atlas and axis.
Figure 3 represents a normal cervical spine as seen from the lateral view. The lordotic curve provides shock absorption, the disc spaces appear to be full and the cervical gravity line, which is located by a point on the anterior third of the odontoid process then drawing a plumb line straight down, represents the center of gravity of the weight of the head (approximately 10% of body weight). In the optimal state, all bones in the neck should share in the distribution of this weight. In Figure 4, the head is grossly anterior to all of the bones in the cervical spine, the spine is straight and the loading of this neck is highly abnormal.
 Fig. 5: Premature Degeneration
In Figure 5, we can see the premature degeneration of the discs at C5, 6 and 7, along with the bony changes at the anterior surface of C5, 6 and 7. This is due to abnormal loading. There is also foraminal encroachment, disc injury, muscular changes, etc. These findings are predictable if the loss of curve and anterior head carriage are not addressed at a younger age.
Fig. 5: Premature Degeneration
In Figure 5, we can see the premature degeneration of the discs at C5, 6 and 7, along with the bony changes at the anterior surface of C5, 6 and 7. This is due to abnormal loading. There is also foraminal encroachment, disc injury, muscular changes, etc. These findings are predictable if the loss of curve and anterior head carriage are not addressed at a younger age.
 Fig. 6: A-P Lumbar
When one side of the pelvis appears much lower than the opposite pelvis, as seen in Figure 6, three considerations must be made; anatomical short leg, increased pronation of the right foot as seen on a digital foot scan or an increased Q angle of the right knee. This differential diagnosis is critical in making the correct recommendations to the young athlete for long term improvement.
Fig. 6: A-P Lumbar
When one side of the pelvis appears much lower than the opposite pelvis, as seen in Figure 6, three considerations must be made; anatomical short leg, increased pronation of the right foot as seen on a digital foot scan or an increased Q angle of the right knee. This differential diagnosis is critical in making the correct recommendations to the young athlete for long term improvement.
Lateral Lumbar
The lateral lumbar provides a wealth of information. Ferguson's gravity line is important, as it represents the athlete's center of gravity from the side. This marking originates in the center of L3, with a plumb line drawn straight downward. This line should bisect the anterior third of the sacral base. In Figure 7, we can see the line falls anterior to the norm. This finding produces increased stresses on the posterior structures of the spine, such as the pars and facets. Dr. Yochum has concluded that no one has ever been born with a pars defect, as pars defects are stress fractures that typically occur during adolescence. The incidence of pars defects increases with extension activities of the low back, as well as with an increased sacral base angle and an anterior Ferguson's gravity line.
 Fig. 7: Anterior Ferguson's Line
In Figure 8, we see Ferguson's gravity line is posterior, suggesting the body's weight bearing is increased over the posterior disc and spinal nerve root. This increased stress, over time, will predictably increase disc injuries and nerve root irritations.
Fig. 7: Anterior Ferguson's Line
In Figure 8, we see Ferguson's gravity line is posterior, suggesting the body's weight bearing is increased over the posterior disc and spinal nerve root. This increased stress, over time, will predictably increase disc injuries and nerve root irritations.
 Fig. 8: Posterior Ferguson's Line
The findings above are just a few that can be determined with the four view series recommended. Without the information found on these x-rays, the provider is reduced to a mere technician treating symptoms. The patient is in charge, as they are the only ones who truly know how well or how poorly they're doing. However, with the x-ray information, combined with a history and all other examination findings, the examiner becomes the true authority and clearly understands in detail what is happening to the athlete's musculoskeletal system. This information allows for a customized corrective program that will help prevent the likelihood for premature breakdown as well as helping the athlete work towards maximum biomechanical improvement. Most importantly, this approach separates an examiner from all other providers in their respective healthcare community.
Fig. 8: Posterior Ferguson's Line
The findings above are just a few that can be determined with the four view series recommended. Without the information found on these x-rays, the provider is reduced to a mere technician treating symptoms. The patient is in charge, as they are the only ones who truly know how well or how poorly they're doing. However, with the x-ray information, combined with a history and all other examination findings, the examiner becomes the true authority and clearly understands in detail what is happening to the athlete's musculoskeletal system. This information allows for a customized corrective program that will help prevent the likelihood for premature breakdown as well as helping the athlete work towards maximum biomechanical improvement. Most importantly, this approach separates an examiner from all other providers in their respective healthcare community.
Editor's Note: This is part three of a six part series by Dr. Maggs. To see parts one and two, visit www.dcpracticeinsights.com.
Dr. Tim Maggs has been in private practice for 35 years and is the developer of The Structural Management® Program and The Concerned Parents of Young Athlete's® Program. He travels the country teaching his program Biomechanics, Imaging and Care of the High School Athlete. For more information, visit www.CPOYA.com.