






Continuity
B.B. Gallaudet1 dissected 34 adult human bodies from 1913-1930 for the sole purpose of examining the fascia in the human body. In the preface of his book, he stated that the "planes of fascia in one region of the body are directly continuous with the same planes in all other regions." He further stated that previous texts had never emphasized the law of continuity of fascial planes.
The Underrated Fascia
In November 2003, I spent four days with Guy Voyer, MD, DO, at Queens University in Kingston, Ottawa. Dr. Voyer has dissected over 100 cadavers, spending most of his time tracing the fascial connections of the body. During this session, I and others spent most of the time watching him dissect and explain the fascial connections in the abdomen and pelvis. A description of the fascial connection between the testicles and skull was included.
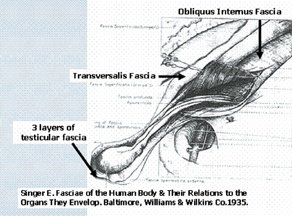
The outer layer of the testicles contains three fascial layers: dartos, scarpa, and Camper's fascia. These layers attach to a conjoined fascial attachment of the obliquus externus and internus and the transversalis fascia; to the thoracic diaphragm fascia; to the middle cervical fascia; to the temporal bone. The middle cervical fascia fuses with the posterior cervical fascia, which attaches to the occipital bone.2,8
It is well-established that fascia forms a continuum throughout the body and surrounds and infuses with every muscle, bone, nerve, blood vessel, organ and cell of the body. Fascial contracture restricts muscular elongation and joint range of motion.3 When a relaxed muscle is physically stretched, it is the connective tissue and sheathing within and around the muscle that offers resistance.4,5
When any joint is restricted over time, it stands to reason that the connective tissue fascia surrounding the joint, and often fascial tissue distant from the joint, will increase its cross-linkage and lose its original shock-absorbing qualities. The status of pre-accident soft tissue is an important reason why some patients suffer for prolonged periods of time after an injury unless the fascial system is released. If a vertebral or extremity fixation does not free up in a reasonable amount of time, we must look to the proximal and distant connective tissue. The fascial system represents an essential element of the kinetic chains many of us look to when local treatment over the painful area is unsatisfactory.
The Fascial Conspirators
Upon viewing the iliac and psoas fascia, I saw a direct connection from this fascia to the peritoneum, diaphragm, kidney, spleen, liver, pancreas, duodenum, sigmoid colon and bladder. In one cadaver, I also noticed the ureter descended over the psoas belly. The iliac fascial connection to the Fallopian tubes may have an indirect effect on the ovaries. There is a direct fascial connection between the apex of the sacrum and the rectum. Tight gluteus medius fascia that attach to the piriformis can cause compression of the superior gluteal vessels and nerve against the piriformis muscle.
In a past article,6 I described lumbar compartment syndromes in which the fascia surrounding the erector spinae restricted normal contraction, resulting in ischemic pain on lumbar flexion or activity. Many times, as a result, fasciotomies are performed.7 Becoming aware of our total bodily connection is the first step in freeing some of us from the "tunnel vision" to which we still adhere.
References
- Gallaudet BB. A Description of the Planes of Fascia of the Human Body. New York, Columbia University Press, 1931(preface).
-
 .
. - Lewit K. Manipulative Therapy in Rehabilitation of the Locomotor System, 2nd ed. Oxford, England, Butterworth/Heinemann, 1991:29.
- Casell C. Tensile force in total striated muscle, isolated fibre and sarcolemma. Acta Physiol Scand 1950;21:380-401.
- Ramsey R, Street S. The isometric length-tension diagram of isolated skeletal muscle fibers of the frog. J Cell Comp Physiol 1940;15:11-34.
- Hammer W. Posterior Spinal Fascial System. Dynamic Chiropractic 2002;20(11).
- Kitajima I, Tachibana S, Hirota Y, Kenichi N. Acute paraspinal muscle compartment syndrome treated with surgical decompression: a case report. Amer J of Sports Med 2002;30(2):283-285.
- Special thanks to publishers Williams and Wilkins for this superb image.
Warren Hammer, MS, DC, DABCO
Norwalk, Connecticut
Click here for previous articles by Warren Hammer, MS, DC, DABCO.