






Patrick's and Hibb's tests are traditionally considered to be tests for hip-joint pathology. However, the pair has also been described as tests for sacroiliac (SI) joint pathology. In reality, the tests can serve both purposes.
Patrick's Test
Patrick's test, also known as the Figure Four or Patrick's FABERE test, is probably the most common test for hip joint pathology. Performed with the patient supine, the test involves placing the patient's coxa joint in flexion, abduction, external rotation and then extension (FABERE). Once the testing leg is in this position, the examiner stabilizes the contralateral anterior-superior iliac spine (ASIS) and gently pushes the testing leg farther into external rotation. (Figure 1)
 FIG 1 Patrick's Testing Position
If the patient is unable to achieve the testing position and/or experiences pain in the hip joint / groin during testing, the test is positive for hip pathology.
FIG 1 Patrick's Testing Position
If the patient is unable to achieve the testing position and/or experiences pain in the hip joint / groin during testing, the test is positive for hip pathology.
When the joint being tested has reached the end of the testing range, the joint capsule is at full tension and the joint itself is in a close-packed position. At this point, the femur and ipsilateral ilium will move together, creating a lever that will stress the ipsilateral sacroiliac joint.
This is when the emphasis of the test transitions from hip joint assessment to sacroiliac joint assessment. Pain in the ipsilateral sacroiliac joint after the transition is a positive test for sacroiliac pathology.
Hibb's Test
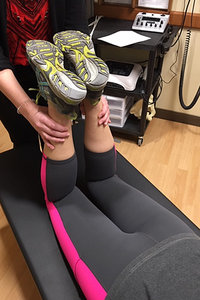 FIG 2A Hibb's Initial Testing Position
Hibb's test, also known as the prone gapping test, is another common test for hip joint pathology. Performed with the patient prone and the knees bent to 90 degrees, the test involves moving the patient's coxa joint from neutral to internal rotation using the lower leg as a lever arm. (Figures 2A and 2B)
FIG 2A Hibb's Initial Testing Position
Hibb's test, also known as the prone gapping test, is another common test for hip joint pathology. Performed with the patient prone and the knees bent to 90 degrees, the test involves moving the patient's coxa joint from neutral to internal rotation using the lower leg as a lever arm. (Figures 2A and 2B)
If the patient is unable to achieve the testing position and/or experiences pain in the hip joint / groin during testing, the test is positive for hip pathology.
When the joint being tested has reached the end of the testing range, the joint capsule is at full tension and the joint itself is in a close-packed position. At this point, the femur and ipsilateral ilium will move together, creating a lever that will stress the ipsilateral sacroiliac joint.
 FIG 2B Hibb's Final Testing Position
This is when the emphasis of the test transitions from hip joint assessment to sacroiliac joint assessment. Pain in the ipsilateral sacroiliac joint after the transition is a positive test for sacroiliac joint pathology.
FIG 2B Hibb's Final Testing Position
This is when the emphasis of the test transitions from hip joint assessment to sacroiliac joint assessment. Pain in the ipsilateral sacroiliac joint after the transition is a positive test for sacroiliac joint pathology.
Test Value, Diagnostic Relevance and Exam Efficiency
Essentially, the mechanisms of the two tests are the same. Using the femur as a lever, initial stress is placed on the hip joint. At the end of the initial testing phase, the femur is joined by the ilium, transitioning stress to the SI joint.
The similarities of the tests make it possible for one test to confirm the results of the other. However, similar does not mean identical or interchangeable. There are subtle differences between the two tests; differences that add value to using the two tests in combination. The added value lies in increased diagnostic relevance and examination efficiency.
In hip joint pathology, internal rotation is typically lost before external rotation. Hibb's assessment uses internal rotation, while Patrick's assessment uses external rotation. This leaves one to wonder why Patrick's test is more widely used. It would be reasonable to assume that Hibb's test would be more sensitive, since it assesses the more frequently lost range of motion. I employ Hibb's test ahead of Patrick's test for this reason.
In terms of efficiency, Hibb's test is performed bilaterally and simultaneously. Patrick's test is performed unilaterally and individually. Thus, Hibb's test requires less time to perform and bilateral comparison is immediately possible.
 FIG 3 Modified Patrick's Testing Position
To improve the efficiency of Patrick's test, I modify its performance. After performing Hibb's test, in which the knees are together (Figure 2A), the thighs are abducted and the lower legs crossed medially to induce external rotation in both hip joints. (Figure 3) The legs are crossed twice, right over left and then left over right. This procedure allows both Hibb's and Patrick's tests to be performed bilaterally and simultaneously without changing the patient's position.
FIG 3 Modified Patrick's Testing Position
To improve the efficiency of Patrick's test, I modify its performance. After performing Hibb's test, in which the knees are together (Figure 2A), the thighs are abducted and the lower legs crossed medially to induce external rotation in both hip joints. (Figure 3) The legs are crossed twice, right over left and then left over right. This procedure allows both Hibb's and Patrick's tests to be performed bilaterally and simultaneously without changing the patient's position.
If the patient can achieve the testing positions for both tests bilaterally and hip / groin or sacroiliac pain are not experienced on either side, both tests are negative. If a testing position cannot be achieved and/or pain is produced, results are positive for the joint being tested on the ipsilateral side. Patrick's test can always be performed in the traditional manner for confirmation of pathological results.
With any clinical testing procedure, the goal is always accuracy of results. This cannot be achieved with Patrick's and Hibb's tests without understanding their testing phases and their relationship to each other for combined use.
Resources
- Gann N. Orthopaedics at a Glance. Thorofare: Slack Incorporated, 2001.
- Ramanurti CP. Orthopaedics in Primary Care. Baltimore: Williams and Wilkins, 1979.
Click here for more information about K. Jeffrey Miller, DC, MBA.