





Case Study #1
History
On November 21, 1991, a 45-year-old male, oil company executive and part-time soccer referee, presented to our office for examination of chronic ankle pain stemming from an ankle injury that had occurred in October 1990.
The patient had been running down a soccer field refereeing a game when he ran into a spectator. At impact they both fell and the patient caught his foot in a way that caused him to suffer a severe inversion sprain to his right ankle. Shortly after the injury he visited an orthopedist who diagnosed a severe inversion sprain and put him in a firm ankle brace for six weeks. After bracing, the patient resumed normal activities and felt that he had essentially recovered at that time although he had never been totally pain free since the original ankle injury. In addition, he has suffered at least two additional inversion sprains since the original injury.
Examination
Gait analysis was essentially normal. No gross or moderate abnormal pronation or supination could be detected visually. Examination of the subtalar and midtarsal joints for weightbearing and nonweightbearing gross alignment also failed to reveal any obvious overall malalignment. Palpation elicited tenderness at the lateral collateral ankle ligaments. Motion palpation of the right foot and ankle elicited stiff, dysfunctional joints: The cuboid joint complex was stiff in inferior to superior "give," "spring" or "joint play" (Fig. 1); the subtalar joint was stiff in axial elongation (traction) and eversion "give," "spring" or "joint play (Fig. 2); and midtarsal joint circumduction stiffness (the general mobility of the forefoot on the rearfoot as elicited by the Hiss test, Fig. 3).

Figure 1: Cuboid-Tarsal Manipulation. With the patient prone, a reinforced thumb contact is made on the cuboid with the fingers wrapping around the dorsum of the foot. A thrust is given laterally and downward.
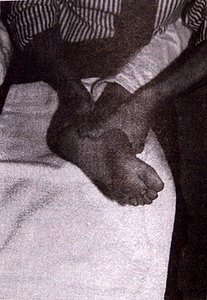
Figure 2: Subtalar Manipulation: The patient's knee is stabilized around the doctor's waist. Each hand wraps around the talus just below the mortise joint. Axial traction is applied, then inversion/eversion movement.
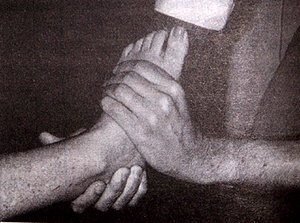
Figure 3: Hiss Test: Forefoot and Midtarsal Examination and Mobilization. With the patient supine, the examiner grasps and stabilizes the rear foot with one hand. The other hand grasps the forefoot and examines motion and mobilizes by circumducting and applying a figure eight motion to the forefoot. The hand positions may be reversed.
Treatment
High velocity, low amplitude manipulation was applied to the cuboid, and low velocity, high amplitude mobilization was applied for: ankle axial elongation (traction), ankle and subtalar eversion, and to the midtarsal (or forefoot/rearfoot) joints in a figure eight pattern (see Figures 1, 2, and 3). Diathermy was used to soften fibrotic tissues and relieve pain. The patient reported relief of the ankle pain after three treatments. After nine treatments, the patient reported 100 percent relief with no pain either on walking or running activities.
Case Study #2
History
A 28-year-old female reported that she was in an automobile accident on August 5, 1985 in which her left knee was injured. The lateral collateral ligaments were severely sprained and initially she was placed in a full leg cast. Later in November, she was still on crutches. She then underwent arthroscopic surgery of the left knee in January 1986. The cast and crutches greatly irritated her spine and her right ankle, and she reported having had progressively worsening ankle pain until she saw a podiatrist in August 1988. The doctor prescribed rigid foot orthotics which reportedly only slightly relieved her ankle pain. On January 19, 1989 she consulted this office for examination and treatment of chronic right ankle pain.
Examination
Gait analysis demonstrated mid-bilateral rearfoot pronation secondary to bilateral nonweightbearing rearfoot varus. There was mild discomfort at the right ankle collateral ligaments on inversion and plantarflexion. Motion palpation of the right foot elicited a stiff cuboid joint complex lacking superior joint play or glide (Fig. 1) along with a stiff first, second and third cuneiform joint complex also lacking superior joint play or glide (Fig. 4). There was also a positive right Hiss test (Fig. 3) generally thought to indicate a stiff foot; a stiff forefoot on the rearfoot as an indicator of a stiff midtarsal joint.
High velocity, low amplitude manipulation was applied to the cuboid, and low velocity, high amplitude mobilization was applied for: ankle axial elongation (traction), ankle and subtalar eversion, and to the midtarsal (or forefoot/rearfoot) joints in a figure eight pattern (see Figures 1, 2, and 3). Diathermy was used to soften fibrotic tissues and relieve pain. The patient reported relief of the ankle pain after three treatments. After nine treatments, the patient reported 100 percent relief with no pain either on walking or running activities. A 28-year-old female reported that she was in an automobile accident on August 5, 1985 in which her left knee was injured. The lateral collateral ligaments were severely sprained and initially she was placed in a full leg cast. Later in November, she was still on crutches. She then underwent arthroscopic surgery of the left knee in January 1986. The cast and crutches greatly irritated her spine and her right ankle, and she reported having had progressively worsening ankle pain until she saw a podiatrist in August 1988. The doctor prescribed rigid foot orthotics which reportedly only slightly relieved her ankle pain. On January 19, 1989 she consulted this office for examination and treatment of chronic right ankle pain. Gait analysis demonstrated mid-bilateral rearfoot pronation secondary to bilateral nonweightbearing rearfoot varus. There was mild discomfort at the right ankle collateral ligaments on inversion and plantarflexion. Motion palpation of the right foot elicited a stiff cuboid joint complex lacking superior joint play or glide (Fig. 1) along with a stiff first, second and third cuneiform joint complex also lacking superior joint play or glide (Fig. 4). There was also a positive right Hiss test (Fig. 3) generally thought to indicate a stiff foot; a stiff forefoot on the rearfoot as an indicator of a stiff midtarsal joint.
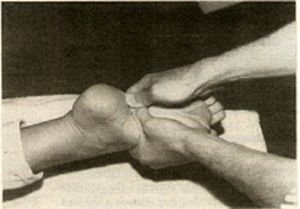
Figure 4: Tarsal Manipulation: As the patient lies prone, a reinforced thumb contact is applied to one of the tarsal bones. A thrust is then given downward while slightly plantar flexing the forefoot.
Treatment
Treatment of the right ankle was instituted on January 19, 1989 and consisted of high velocity, low amplitude manipulation to the right cuboid joint complex (Fig. 1), second and third cuneiform joint complex (Fig. 4), and a figure eight low velocity, high amplitude mobilization of the forefoot on the rearfoot (for mobilization of the midtarsal joint (Figure 3). After four treatments she reported 50 percent relief, and after 12 treatments she reported over 90 percent relief. Contacted over two years later, she reports that her ankle pain relief has remained at 90 percent.
Discussion -- Joint Dysfunction As a Cause of Unresolved Ankle Pain
Hiss ran a large foot clinic which emphasized osteopathic foot manipulation and wrote that unrecognized joint dysfunction as the major cause of unresolved ankle sprain.8 He came to view the "sprained ankle" as mostly a foot injury to the calcaneal-cuboid joint, and to a lesser degree the other intertarsal joints. Hiss felt that the resulting tarsal joint dysfunction was responsible for chronic ankle pain and would only respond to appropriate manipulation.8
James Mennell, a physiatrist, wrote that in the process of an ankle inversion sprain, foot joints are also injured and that the manipulation of these other foot joints is necessary to fully relieve the pain of an ankle sprain.9,10 John Mennell, Schafer, Faye, and Michaud have all written on the need to diagnose and treat foot joint dysfunction to more fully manage and relieve ankle pain.3,4,11 Subotnick, a podiarist, published a textbook on Sports Medicine Injuries to the Lower Extremities which included a chapter on foot and ankle manipulation. In this textbook he suggested that intertarsal joints are often injured in ankle sprains and should have manipulative diagnosis and treatment to more effectively relieve the after effects of an ankle sprain.6
The primary intertarsal joints injured in ankle sprains most often cited in the literature are the cuboid and its articulations and the cuneiforms and their articulations.4,8,9 The subtalar joint is the next most mentioned intertarsal joint cited.4,11 The ankle joint itself may become dysfunctional and partially or wholly become hypomobile.4,6
Summary
Tarsal joints may be injured an sprained at the same time that an ankle sprain occurs. In another visualization, the sprained ankle, made slightly hypermobile or loose, may produce secondary or compensating hypomobile or stiff tarsal joints. Both scenarios may produce painful dysfunctional tarsal joints that refer pain to the ankle mortise in spite of appropriate therapy directed at the ankle or in spite of orthotic therapy to correct excessive pronation or deformity. In such cases, chiropractic manipulative foot care to treat hypomobile, dysfunctional foot and ankle joints is indicated and effective.
References
- Calliet R: Foot and Ankle Pain. Philadelphia: FA Davis, 129-31, 1968.
- Yale JF: Podiatric Medicine, ed 3. Baltimore, MD: Williams and Wilkins Co., 276-81, 1980.
- Michaud TC: Aberrancy of the midtarsal locking mechanism as a causative factor in recurrent ankle sprains. JMPT, 2:135-144, 1989.
- Schafer RC and Faye LJ: Motion Palpation and Chiropractic Technique, ed 1. Huntington Beach, California. The Motion Palpation Institute, 1989.
- Levy LA and Hetherington VJ: Principles and Practice of Podiatric Medicine. New York, Churchill Livingstone, 1990.
- Subotnick SI: Sports Medicine of the Lower Extremity. Editor: Subotnick SI: New York. Churchill Livingstone, 1989.
- Root ML, Oriend WP, and Weed JH: Normal and abnormal function of the foot. Los Angeles, CA: Clinical Biomechanics Corp., 322-5, 1977.
- Hiss JM: Functional Foot Disorders, ed 3. Los Angeles, CA: The Oxford Press, 307-21, l949.
- Mennell J: Physical Treatment by Movement Manipulation and Massage, ed 4. Philadelphia: The Blakiston Co., 1940.
- Mennell J: The Science and Art of Joint Manipulation. Philadelphia: The Blakiston Co., (James), 1949.
- Mennell JM: Foot Pain. Boston: Little, Brown and Co., 1969.
James Brantingham, D.C.
Randy Snyder, D.C.
John Wong, D.P.M., D.C.
Charles Brantingham, D.P.M.
Bruce Haggart, D.C.
Tarzana, California