





We have all experienced patients with an uncomplicated lesion or misalignment of the sacroiliac joint whose complaints were not resolved with even the best care we could render using conventional diagnostic and adjusting strategies.
At least part of the answer to the problem of these so-called atypical presentations of LBP with sacroiliac involvement may lie outside the assumptions and thinking framework many of us have learned to use. The concept that pain, symptoms and other clinical findings are a result of interosseous positional relationships may not tell the whole story.
The Tensegrity Matrix
Roth explores the tensegrity matrix model to help explain the recurrent and chronic conditions. Tensegrity, a term coined by Buckminister Fuller, describes the tensional, integrity and functional relationship of "all the structural component[s] of the body."1
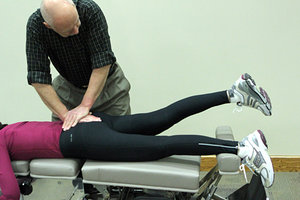 Sacral leg check.
Roth argues, "Symptoms, especially in chronic conditions, are often the result of the compensatory tensions and stresses created within the body in response to a primary site of injury ... diagnosis and treatment based on the area of symptoms, is often frustrating and fruitless since it acts only on the peripheral effects of the primary condition."1
Sacral leg check.
Roth argues, "Symptoms, especially in chronic conditions, are often the result of the compensatory tensions and stresses created within the body in response to a primary site of injury ... diagnosis and treatment based on the area of symptoms, is often frustrating and fruitless since it acts only on the peripheral effects of the primary condition."1
Schleip also observes fascial response to inflammation and injury may provide another explanation for SI dysfunction without measurable radiographic evidence of misalignment. "The presence of myofibroblasts in skeletal ligaments and tendons," Schleip suggests, may result in reduced distensability of articular and periarticular soft tissue4 with fixation, adhesion and reduced ROM. Fibrotic adhesions may reach "pathological proportions," Schleip observes, with a negative impact on the soft-tissue network of the pelvic articulations.
Recent studies in the anatomical soft tissue matrix, Roth observes, "[E]xtend the basic concept of tissue response to injury ... to include all structures of the body."2 In fact, a growing body of basic research into the role of connective tissue may suggest why our "problematic" patients – particularly those with recurrent and chronic presentations – experience their difficulties.
Langevin, who has developed a body of seminal literature based on her connective-tissue research, comments, "This network is so extensive and ubiquitous that if we were to lose every organ, muscle, bone, nerve, and blood vessel in our bodies, we would still maintain the same shape: our ‘connective-tissue body.'"2
 Sacral apex right adjustment.
Some might recall the biology class response to this observation: "We'd be dead!" but Langevin also contributes to the understanding of what may be happening with recurrent LBP and misalignments of the sacroiliac joints, the sacrum and the lumbosacral junction. If we look at the pelvic motor units as suspended in a framework of both osseous and soft tissue, we can visualize not only the biomechanics of stressors to the region, but also the virtually instantaneous communication within the tensional framework.
Sacral apex right adjustment.
Some might recall the biology class response to this observation: "We'd be dead!" but Langevin also contributes to the understanding of what may be happening with recurrent LBP and misalignments of the sacroiliac joints, the sacrum and the lumbosacral junction. If we look at the pelvic motor units as suspended in a framework of both osseous and soft tissue, we can visualize not only the biomechanics of stressors to the region, but also the virtually instantaneous communication within the tensional framework.
Application: Recurrent LBP With SI Misalignments
Let us consider, for example, a patient who demonstrates low back pain which can be traced to a sacral misalignment. We suggest that sacral involvement induces stressors into the soft-tissue network of the pelvis – interosseous, sacrotuberous, and sacrospinalis ligaments and surrounding fascial matrix. Thus, dysfunction and symptoms are more a consequence of asymmetry and imbalance within the soft-tissue framework of the pelvis, rather than osseous misalignment.
As Roth points out, "A primary restriction in one location will transmit a certain amount of tension throughout the entire body, producing a background level of tension we refer to as the tissue barrier. Changing the primary restriction should, in turn, change the tissue barrier."1
Sacral apex deviation (+/- ΘZ) is a good example of a perturbation of the tensegrity framework. As a follow-up to a positive or negative Derifield test and correction of the sacroiliac joints, especially for patients with atypical low back pain originating in persistent pelvic joint symptoms, perform a sacral leg check using the protocol developed by Thompson.3 The test is essentially an active range-of-motion assessment of thigh extension associated with the sacrum within its soft-tissue framework.
The Assessment
To test the prone patient for sacral apex deviation (SAL/SAR,) take a straightaway stance at the level of the sacrum. Place the heel of the superior hand firmly on the sacral base and stabilize with the inferior hand over the dorsum of the contact hand. This stabilization is critical to prevent the ASISs from leaving the table.
Instruct the patient to lock the knee on one side and lift the leg into extension as far as possible, hold briefly and then lower the leg. Note the height of the foot from the table. Next, instruct the patient to lock the knee on the other side and lift that leg into extension until resistance is felt, hold briefly and then lower the leg. Remind the patient that this is not a strength test, but active ROM.
If one leg raises more than 6 inches higher than the other, the test indicates sacral apex deviation to the higher-leg side. If the left leg lifts higher, the test indicates a sacral apex left (SAL;) and if the right leg lifts higher, the test indicates a sacral apex right (SAR.)
The Correction
To adjust sacral apex deviation, cross the patient's thigh on the side opposite apex deviation over the thigh on the side of apex deviation. Assume a scissors stance on the side opposite the misalignment, facing superiorly – e.g., stand on the patient's left side for an SAR correction.
Use a pisiform contact with the inferior hand on the sacral notch on the side of apical deviation. At the same time, take a pisiform contact with the superior hand on the medial aspect of the PSIS on the side of apex deviation. Apply a thrust simultaneously with both hands.
The net effect of the paired thrusts is to induce a corrective torque to the sacrum – clockwise for an SAR and counterclockwise for an SAL.
A post-adjustment sacral leg check typically shows that the legs lift equally, indicating resolution of the sacral misalignment. The effect of the adjustment is to abate the "tissue barrier"1 created by the background level of asymmetrical tension and imbalance within the soft-tissue framework of the pelvis. It also remediates the asymmetrical tension created by the fibrocytic activity Schleip observes. Consequently, the patient enjoys a reduction of symptoms and an increase in mobility of pelvic articulations.
References
- Roth GB. "Matrix Repatterning: The Structural Basis of Health." Matrix Repatterning: www.matrixrepatterning.com/Pr_MR_article.
- Langevin H. "The Science of Stretch." The Scientist, May 1, 2013.
- Thompson Educational Workshops. The Thompson Technique Reference Manual. Elgin, IL: 1984.
- Schleip,R, et al. Fascia: The Tensional Network of the Human Body. Churchill-Livington, Elsevier, 2011.
Dr. Howard Pettersson, a 1976 graduate of Logan College of Chiropractic, is an associate professor of technique at Palmer College of Chiropractic. He was the senior editor of Activator Methods Chiropractic Technique – College Edition, published in 1989, and published Pelvic Drop Table Adjusting Technique in 1999. His most recent publication, written with Dr. Green, is How to Find a Subluxation, published in 2003.
Dr. J.R. Green is a 1988 Graduate of Palmer College of Chiropractic. He retired from the Palmer faculty after many years of teaching basic sciences and chiropractic technique. He is currently in private practice in Galva, Ill., and is also an adjunct professor of chemistry with the Eastern Iowa Community College District. Dr. Green was one of the writers of Activator Methods Chiropractic Technique (1997) and also worked as a technical writing consultant on Activator Methods Chiropractic Technique – College Edition and Pelvic Drop Table Adjusting Technique.